

Why Nasal Sprays Might Not Be Fixing Your Breathing
You’ve tried the spray. Maybe you’ve also tried nasal strips, a humidifier, and sleeping propped up. And yet your nose still feels blocked—especially at night or during workouts. If you continue to wonder why your nasal spray isn’t working, you’re not alone.
Nasal sprays can be helpful, but they’re not a cure-all. When they fail, it’s often because the technique is off, the type of spray doesn’t match the problem, the spray is being overused (leading to rebound congestion), or the real issue is structural (like a deviated septum or nasal obstruction). This post breaks down the most common reasons sprays don’t deliver, how to use them correctly, red flags to watch for, and what to do next—especially if chronic nasal congestion is affecting sleep and quality of life. (Cleveland Clinic; Cure Allergy Clinic; Jacksonville Breathe Free)
When a Nasal Spray Should Help (and what “help” looks like)
What most sprays can realistically do
Different sprays do different jobs. In general, nasal sprays may:
- Reduce swelling/inflammation (common with steroid sprays)
- Thin mucus and moisturize (saline sprays/rinses)
- Temporarily shrink blood vessels to open airflow (decongestant sprays)
A useful way to think about this: saline is like rinsing and hydrating, steroids are like calming an irritated lining over time, and decongestants are like a temporary “quick-open” button. The key is setting expectations: sprays often reduce symptoms, but they may not fix the underlying cause—especially if anatomy is driving the blockage. (Cleveland Clinic)
Signs your spray is working vs. signs it’s masking a bigger problem
More likely working:
- Airflow improves gradually (especially with steroid sprays)
- Symptoms stay improved when used as directed
- You need it less, not more, over time
Potentially masking a larger underlying issue:
- Relief lasts only a short time
- You find yourself reaching for the spray more often
- Symptoms rebound quickly when you stop (Jacksonville Breathe Free)
If you continue to wonder why your nasal spray isn’t working even after consistent, correct use, it’s time to look beyond “stronger medicine” and consider whether the target (inflammation vs. dryness vs. structure) is being missed.
Setting the right expectations—and matching the tool to the cause—often determines whether a spray truly helps.

Reason #1 — Technique Problems: The Medicine Isn’t Reaching Where It Needs to Go
The most common application mistakes
Many sprays “fail” because they’re not landing on the right tissue. If medication hits the septum (the middle wall) or drains straight down the throat, it may irritate without actually treating the swollen areas that narrow airflow.
Common mistakes include:
- Spraying straight up instead of aiming slightly outward
- Sniffing forcefully, pulling medication into the throat
- Not clearing the nose first, so mucus blocks delivery
- Pointing toward the septum, which can increase irritation and nosebleeds (Cleveland Clinic; Cure Allergy Clinic)
A common real-life example: someone sprays, takes a big sniff, tastes the medicine immediately—and assumes that taste means “it worked.” In reality, that strong taste can mean the medicine never stayed where it was needed.
“How to use nasal spray correctly” (quick checklist)
Use this simple routine to improve results:
1. Gently blow your nose (if needed).
2. Keep your head neutral or slightly forward (not tipped far back).
3. Insert the nozzle and aim outward—toward the ear on the same side (away from the septum).
4. Spray while taking a gentle inhale (avoid a “power sniff”).
5. Don’t blow your nose immediately afterward. (Cleveland Clinic; Cure Allergy Clinic)
A useful mnemonic: aim away from the middle, sniff like you’re smelling soup—not like you’re trying to inhale it.
Small technique tweaks often turn “this doesn’t work” into “this finally helps.”

Reason #2 — You’re Using the Wrong Type of Spray for Your Problem
The main categories (in plain English)
Here’s the big-picture difference between common options (Cleveland Clinic):
- Saline sprays/rinses: Hydrate tissues and help clear mucus; generally safe long-term.
- Steroid sprays: Reduce inflammation (often helpful for allergies and ongoing swelling); not instant.
- Antihistamine sprays: Help when symptoms are allergy-driven.
- Decongestant sprays: Fast opening of nasal passages, but meant for short-term use only.
This is where saline spray vs steroid spray becomes a practical decision: saline helps rinse and moisturize, while steroids target inflammation over time. If your nose feels dry, crusty, and sticky, saline may do more than you expect. If your symptoms track with allergy seasons or dust exposure, an anti-inflammatory approach may matter more. For help sorting inflammation vs anatomy, see deviated septum vs allergies: how to tell the difference: https://www.clearpathnasal.com/blog/deviated-septum-vs-allergies-how-to-tell-the-difference
Timing mismatch: why some sprays feel like they “don’t work”
A very common reason for perceived nasal spray failure is expecting immediate results, particularly with steroid sprays, which require consistent daily use for several days to achieve benefit. Decongestant sprays work quickly, but if your main issue is inflammation that needs steady control—or a deviated septum causing nasal obstruction—quick relief may be limited or short-lived. (Cleveland Clinic; Jacksonville Breathe Free)
A concrete example: if your congestion is worst at night, it’s easy to assume you need the “fastest” option. But nighttime blockage can also reflect chronic swelling, dryness, or structure—things a short-acting spray may not solve for long.
Choose the right category—and timeline—for your specific problem to avoid disappointment.

Reason #3 — Overuse Can Cause Rebound Congestion (and Dependence)
What rebound congestion is
With decongestant sprays, overuse can cause rebound congestion—a condition where the nasal lining becomes more swollen when the medication wears off, creating a cycle where you feel like you must keep spraying to breathe. Most labels limit decongestant sprays to only a few days of use; always check instructions and ask a clinician if unsure. (Jacksonville Breathe Free)
Over time, this pattern can resemble nasal spray dependency, where stopping feels difficult because congestion flares strongly at first. People often describe it like this: “I used it to get through one bad night… and now I can’t sleep without it.” Professional guidance is recommended rather than trying to push through alone.
Red flags you may be stuck in rebound congestion
Consider rebound congestion if:
- You need the spray multiple times daily
- The relief lasts shorter and shorter
- Congestion feels worse without it (Jacksonville Breathe Free)
What to do if you suspect rebound congestion
- Get guidance from a clinician on stopping or tapering safely.
- Ask about saline routines and whether a clinician-directed plan (often including anti-inflammatory options) makes sense while your nose resets.
- Seek prompt care if you have significant bleeding, severe obstruction, or concerning side effects. (Cleveland Clinic; Jacksonville Breathe Free)
If you’re overusing a decongestant spray, medical guidance can help you taper and break the cycle safely.

Reason #4 — Sprays Don’t Fix Structural Blockages (Like a Deviated Septum)
Anatomy problems that sprays can’t “shrink away”
Some nasal obstruction is mechanical. Sprays can reduce swelling, but they can’t reliably correct:
- Deviated septum
- Narrowing at the nasal valve area
- Turbinate enlargement that isn’t primarily temporary inflammation
Clues that structure may be the real issue
- One-sided blockage most days
- Chronic mouth breathing
- Symptoms that persist despite appropriate medication use (Jacksonville Breathe Free)
This is often where people feel most frustrated: you can do everything “right,” but if airflow is physically pinched, medication may offer only partial relief. If you suspect this, you may find this helpful: deviated septum explained: https://www.clearpathnasal.com/blog/deviated-septum-explained-symptoms-causes-and-modern-treatment-options
When evaluation matters more than another medication
When symptoms are persistent, an ENT evaluation can clarify whether chronic nasal congestion is driven by inflammation, anatomy, or both. This isn’t about failing sprays—it’s about matching treatment to the cause. Decisions about procedures should always be clinician-guided. (Jacksonville Breathe Free)
If structure is the roadblock, evaluation—not another bottle—opens the door to real solutions.

Reason #5 — For Some Conditions, Sprays May Be No Better Than Saline
Example: sleep-disordered breathing (especially in children) and medication limits
In certain pediatric sleep-disordered breathing contexts, research suggests medicated sprays may not clearly outperform simple saline for symptom improvement—highlighting that medication is not always the deciding factor when obstruction and sleep are involved. (Oxford Academic, Sleep Advances; PMC review)
What this means for patients/parents
If snoring, restless sleep, or daytime fatigue continues, it’s worth assessing the whole picture—nasal obstruction, allergies, and (in children) common contributors like tonsils/adenoids—rather than relying on a spray alone. (Oxford Academic; PMC)
When sleep and airflow are involved, look beyond the bottle to the broader causes.
Burning, Stinging, or Irritation: A Clue Your Nose Needs a Different Approach
Common reasons sprays burn
Burning can happen when:
- The nasal lining is inflamed or dry
- The nozzle is angled toward the septum
- You’re sensitive to an ingredient (Cleveland Clinic; Cure Allergy Clinic)
If your nose feels like it “catches fire” after each use, that’s a signal—not something to power through indefinitely.
Practical next steps
- Re-check your angle and routine using the checklist above.
- Consider switching to gentler saline support.
- If irritation persists or bleeding develops, discuss alternatives with a clinician. (Cleveland Clinic)
Stinging or bleeding is feedback—adjust the technique or the plan with professional help.
If Sprays Aren’t Enough: Long-Term Options That Target the Root Cause
Conservative options to discuss first
Before considering procedures, many people benefit from:
- Regular saline irrigation habits
- Allergy evaluation/management if symptoms fit
- Reducing triggers like smoke, dry air, and irritants (Cleveland Clinic; Jacksonville Breathe Free)
You may also find it useful to compare symptoms with deviated septum vs allergies: how to tell the difference: https://www.clearpathnasal.com/blog/deviated-septum-vs-allergies-how-to-tell-the-difference
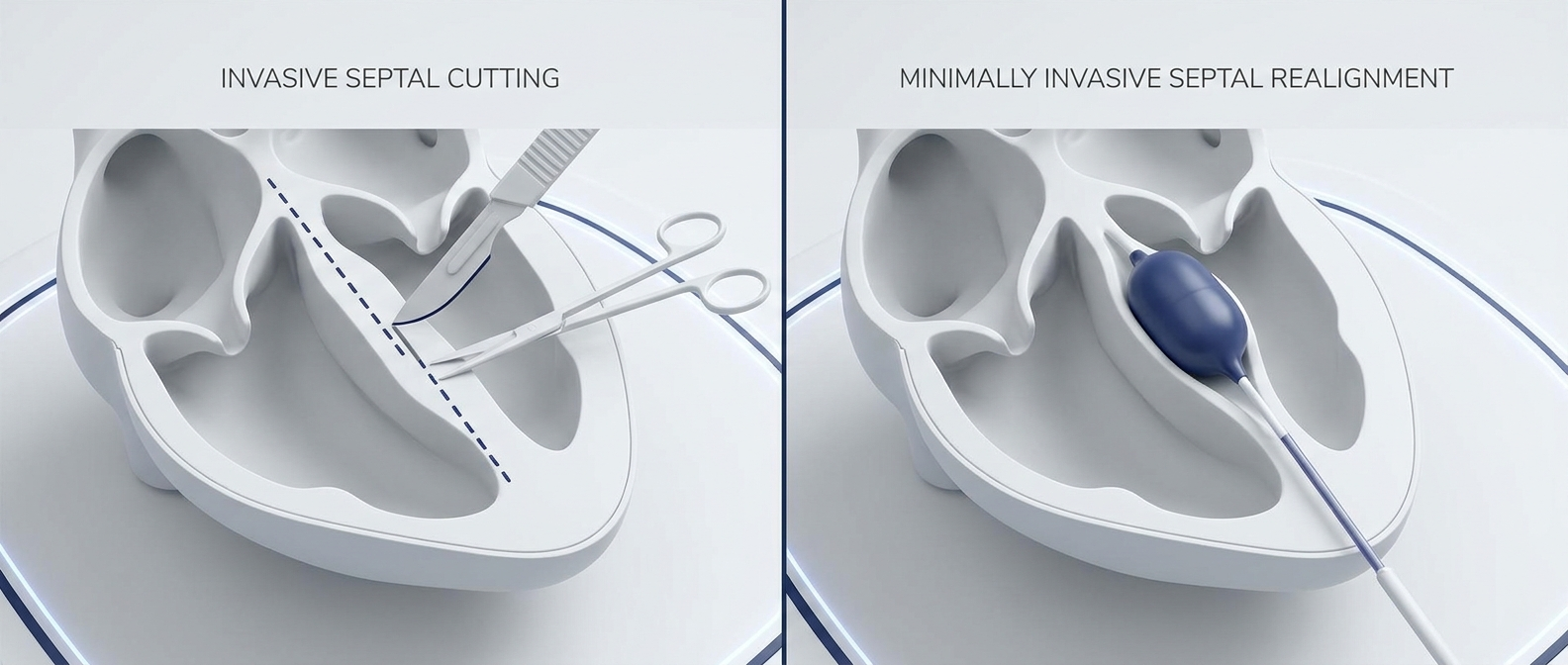
When a minimally invasive structural solution may help
If the underlying issue is structural—especially a deviated septum—medication may never fully solve the airflow problem. In those cases, a clinician may discuss procedural options, including balloon septoplasty approaches, designed to address anatomy rather than escalating daily sprays. A patient-friendly overview is here: what is balloon septoplasty?: https://www.clearpathnasal.com/blog/what-is-balloon-septoplasty-a-minimally-invasive-option-for-deviated-septum
ClearPath Nasal Balloon (CNB) + balloon-assisted endoscopic septoplasty (key evidence points)
One newer approach uses the ClearPath Nasal Balloon (CNB)—a device used in balloon-assisted endoscopic septoplasty. In a retrospective series of 107 cases, early outcomes reported included:
- Safety: No major complications such as septal perforation, hematoma, mucosal injury, or synechia were observed.
- Symptoms: Average SNOT-22 decreased ~24%, including improvement in congestion, facial pressure, and sleep quality at 1 month.
- Imaging subset: Mean improvement of 45% at maximal deviation and 22% at the nasolacrimal duct (both p=0.005).
- Efficiency potential: The technique may reduce steps like packing/suturing and potentially shorten anesthesia time. (Dillard JD, Koudouovoh C, Lee V, et al. Rhinology Online. 2026;9:18–23. doi:10.4193/RHINOL/25.018)
These data are from a retrospective series and should be viewed as preliminary; availability, candidacy, and outcomes vary. For a visual walkthrough, see how the ClearPath Nasal Balloon works (step-by-step): https://www.clearpathnasal.com/blog/how-the-clearpath-nasal-balloon-works-a-step-by-step-guide. If you’re comparing options, this may help: ClearPath vs traditional septoplasty: https://www.clearpathnasal.com/blog/clearpath-vs-traditional-septoplasty-recovery-safety-results. Surgical decisions should always be made with your ENT based on your specific anatomy and goals.
Start with conservative care, then consider minimally invasive structural options—guided by an ENT who knows your anatomy.
When to See a Clinician (and what to ask)
Make an appointment if…
Consider evaluation if:
- Symptoms last more than 2–4 weeks despite correct use
- One-sided blockage happens most days
- Frequent sinus infections, nosebleeds, facial pressure, or reduced smell
- You suspect nasal spray rebound congestion
- Snoring or sleep disruption with daytime fatigue (Cleveland Clinic; Jacksonville Breathe Free)
Questions to bring to an ENT visit
- Could this be structural (septum/turbinates/valve)?
- Am I using the right spray—and using it correctly?
- Could rebound congestion be involved?
- What options exist beyond daily sprays?
- If a procedure is on the table, is a minimally invasive option (like balloon-assisted endoscopic septoplasty) appropriate—and should we discuss devices such as ClearPath as an alternative to more traditional approaches? (Cleveland Clinic)
Timely evaluation can save months of trial-and-error and point you to the right plan faster.
FAQ
Why does my nasal spray work for a few hours and then stop?
Often it’s because the spray is a short-acting decongestant, or because ongoing inflammation/structural nasal obstruction is still there once the medication wears off. (Cleveland Clinic; Jacksonville Breathe Free)
Can I use decongestant spray every day?
Daily long-term use is generally discouraged due to rebound congestion risk; most labels limit use to a few days. Ask a clinician if you’re unsure. (Jacksonville Breathe Free)
Is saline “strong enough”?
In some situations, yes—especially for moisturizing and mucus clearance, and some research contexts suggest saline may perform similarly to medicated sprays for certain symptoms. (Oxford Academic; PMC)
How do I know if I have a deviated septum?
Common clues include persistent one-sided obstruction and chronic mouth breathing, but diagnosis requires an exam. (Jacksonville Breathe Free)
Conclusion
If you’re stuck on why your nasal spray isn’t working, the answer is often one of five things: technique errors, the wrong spray type (or wrong timeline), rebound congestion from overuse, irritation/dryness, or a structural problem like a deviated septum causing chronic nasal obstruction.
Try tightening up technique, match the spray to the problem, and avoid overusing decongestants. But don’t ignore persistent symptoms—especially sleep disruption and one-sided blockage.
CTA: If congestion has become your “normal,” schedule an evaluation with your local ENT and ask whether your symptoms point to inflammation, structure, or both—and whether minimally invasive options (including balloon-assisted approaches such as ClearPath) make sense for you.
References
- Cleveland Clinic. “How to Use Nasal Spray.” https://health.clevelandclinic.org/how-to-use-nasal-spray
- Cure Allergy Clinic. “How to Use Nasal Spray Correctly.” https://cureallergyclinic.com/how-to-use-nasal-spray-correctly/
- Jacksonville Breathe Free. “Is it Time to Ditch the Nasal Spray? Long-Term Solutions for Better Breathing.” https://www.jacksonvillebreathefree.com/blog/is-it-time-to-ditch-the-nasal-spray-long-term-solutions-for-better-breathing/
- PMC (NCBI). Review article (nasal obstruction/sleep context). https://pmc.ncbi.nlm.nih.gov/articles/PMC9857783/
- Oxford Academic, Sleep Advances abstract. https://academic.oup.com/sleepadvances/article/6/Supplement_1/A5/8271603
- Dillard JD, Koudouovoh C, Lee V, et al. Rhinology Online. 2026;9:18–23. doi:10.4193/RHINOL/25.018
Disclaimer
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.