
Why Does My Nose Bleed? Could It Be a Deviated Septum?
If you’ve been wondering, “Why does my nose bleed—deviated septum?” you’re not alone. Nosebleeds are common, and a deviated septum can be part of the story—but it’s often not the whole story.
Think of it this way: the inside of the nose is lined with delicate mucosa (the nasal lining). When that lining gets dry, inflamed, or repeatedly bumped, it can bleed surprisingly easily.
Quick answer (and why it’s not always your septum)
A deviated septum can contribute to nosebleeds by changing airflow in the nose, which may dry and irritate the nasal lining, and sometimes by creating small areas of repeated trauma (for example, from crusting or a septal spur). Major clinical resources list a deviated septum as a possible contributor to nosebleeds—among many other common causes. But here’s the important nuance: many people with a deviated septum never develop nosebleeds, and septal deviation is very common in the general population.
So if you’re asking “why does my nose bleed—deviated septum or something else?”, the best next step is to consider the full checklist of triggers—not just anatomy.
*Bottom line: a deviated septum can play a role, but dryness, irritation, and other triggers are often the main drivers.*
What a nosebleed (epistaxis) really is

Why the nose bleeds so easily
The inside of your nose has a thin, delicate lining and a dense network of small blood vessels, especially toward the front of the nose. That’s why even minor irritation—dry air, rubbing, a cold—can set off bleeding. Most nosebleeds start in the front of the nose and can be managed at home.
Occasional vs. recurrent nosebleeds
An occasional nosebleed can happen to anyone—after a stuffy night, a long flight, or a week of allergies. Recurrent nosebleeds are nosebleeds that happen repeatedly over time. Examples include:
- episodes several times a month
- repeated bleeds from the same nostril
- bleeds that are hard to stop
- episodes that disrupt sleep, work, or daily routines
When nosebleeds become recurrent, it’s time for a more systematic look at causes—rather than assuming the answer is automatically “deviated septum.”
*If nosebleeds keep happening, broaden the search for causes beyond the septum.*
Common reasons for nosebleeds (do these first)

Before concluding “why does my nose bleed—deviated septum?”, it helps to rule out the most common, most fixable triggers.
Dry air and low humidity (most common trigger)
Dryness is a big one—especially with:
- heated indoor air in winter
- dry climates
- air travel
Helpful basics:
- a bedroom humidifier
- saline spray (or gentle saline rinses if tolerated)
- a nasal moisturizing gel applied just inside the nostrils
Concrete example: If you wake up with a dry mouth, scratchy throat, and crusty nostrils during winter heating season, that same dryness may be setting you up for small cracks in the nasal lining.
Irritation/trauma
Common causes include:
- nose picking (even occasional)
- forceful blowing
- frequent swabbing
- contact sports or minor bumps
Even well‑intended habits can matter. For instance, repeatedly “checking” a tender spot with a tissue can keep reopening the same tiny vessel—similar to how a scab on your knuckle keeps splitting if it’s constantly bent.
Medications and supplements that increase bleeding risk
Some medicines can make bleeding more likely, including:
- anticoagulants (“blood thinners”)
- aspirin
- NSAIDs (like ibuprofen/naproxen)
Don’t stop a prescribed blood thinner without talking to your clinician.
Inflammation and illness
Colds, allergies, and other nasal inflammation can make the lining more fragile, which increases bleeding risk. If your nosebleeds cluster around allergy flare‑ups—more sneezing, more rubbing, more blowing—that pattern can be a useful clue.
Less common but important medical causes
Less commonly, recurrent nosebleeds can be related to medical issues such as uncontrolled high blood pressure or bleeding/clotting disorders. In certain situations, your clinician may recommend bloodwork.
*Start with dryness, irritation, and medication review—because fixing these often reduces nosebleeds quickly.*
What is a deviated septum (and how common is it)?
The septum in plain language
Your nasal septum is the “wall” that separates the left and right nostrils. A deviated septum means that wall is off‑center or has areas that curve or narrow one side.
Deviated septum is common
Some studies, depending on how septal deviation is defined, report high prevalence rates—sometimes around 86%. Many people with a deviated septum have no symptoms at all.
Symptoms that often travel together
- one‑sided nasal blockage
- chronic congestion
- crusting
- noisy breathing
- sleep disruption
For a deeper overview, see: deviated septum symptoms, causes, and treatment options: https://www.clearpathnasal.com/blog/deviated-septum-explained-symptoms-causes-and-modern-treatment-options
Readers who also struggle with stuffiness may find: deviated septum and chronic nasal congestion: https://www.clearpathnasal.com/blog/deviated-septum-and-chronic-nasal-congestion-what-to-do-next
*A deviated septum is common; it matters most when it lines up with ongoing blockage, crusting, or one‑sided symptoms.*
The deviated septum–nosebleed connection (what’s the mechanism?)

If you keep thinking “why does my nose bleed—deviated septum?”, these are the most commonly discussed ways septal deviation may contribute.
1) Altered airflow can dry out the lining
A deviated septum can create uneven or turbulent airflow, so certain areas dry out more than others. Dry lining can crack and become irritated, making those superficial blood vessels easier to break.
Analogy: It’s a bit like a windy doorway that dries out one corner of a room faster than the rest—one small area takes the hit repeatedly.
2) Crusting leads to repeat irritation (a “scratch‑and‑bleed” cycle)
Dryness often leads to crusting. Crusts feel irritating, so people rub, pick, or blow more often—reopening the same fragile spot and triggering repeat bleeding.
A common pattern is: dry nose → crust → “I’ll just clear this out” → a small bleed → more crusting later → repeat.
3) Septal spurs can cause localized trauma
Some deviations include septal spurs—bony or cartilaginous projections that may irritate nearby tissue. That localized irritation can make bleeding more likely in a specific area.
4) Ongoing local inflammation may weaken superficial vessels
Chronic irritation and inflammation can make the nasal lining more fragile over time.
*A deviated septum may set the stage for dryness and irritation, but it’s usually one factor among several.*
Why a deviated septum isn’t automatically the cause of your nosebleeds
“Common condition” doesn’t equal “confirmed cause”
Because septal deviation is so common, finding one doesn’t automatically explain bleeding—many people have deviation and never experience epistaxis. In other words, a deviated septum can be a meaningful piece of the puzzle without being the main driver.
What makes the septum more suspicious as a contributor?
- bleeding happens repeatedly from the same side
- there’s visible crusting/dryness mostly in one nostril
- you’ve also had long‑term one‑sided obstruction or irritation
Even then, an exam is usually needed to confirm what’s actually bleeding.
*Don’t stop at “I have a deviation”—focus on patterns, one‑sidedness, and what the exam shows.*
What to do during a nosebleed (safe at‑home steps)

Step‑by‑step first aid
Many ENT sources recommend:
1. Sit upright and lean forward (so you don’t swallow blood).
2. Pinch the soft part of your nose (not the bony bridge).
3. Hold steady pressure continuously for a timed interval—avoid checking every few seconds.
A practical tip: set a timer. Many “won’t stop” nosebleeds are actually stopping and restarting because pressure is released too soon.
What not to do
- Don’t tilt your head back.
- Don’t repeatedly release pressure to “see if it stopped.”
- Avoid deep, improvised packing with tissues unless you’ve been instructed.
*Good technique—steady pressure, leaning forward—often makes the biggest difference.*
How to reduce repeat nosebleeds if dryness is the trigger

Moisture strategy (simple routine)
A simple approach many people can stick with:
- saline spray as needed (or gentle saline rinse if comfortable)
- a nasal gel/ointment applied near the front of the nostrils
- aim for comfortable bedroom humidity (often around 30–50%, depending on comfort and home conditions)
Consistency matters more than intensity—small, regular moisture tends to work better than occasional “big” interventions.
Habit and environment checks
- Blow gently.
- Reduce picking/rubbing triggers (trim nails for kids).
- Address allergy triggers and indoor irritants.
- If you’re on a prescribed blood thinner, ask your clinician before changing anything.
*Gentle habits and steady moisture usually lower the odds of repeat bleeds.*
When to seek urgent care vs. schedule an ENT visit
Get urgent/emergency help if:
- bleeding is heavy or won’t stop after correct pressure
- you feel faint or unwell
- bleeding follows significant injury
- you’re coughing or vomiting large amounts of blood
Consider an ENT appointment if:
- nosebleeds are frequent or recurrent
- you also have chronic one‑sided blockage/crusting (and suspect deviation)
- bleeds continue despite humidification and moisture routines
*Seek urgent care for heavy or unrelenting bleeding; see an ENT for patterns that keep coming back.*
How doctors figure out what’s causing recurrent nosebleeds
History: your “pattern” matters
A clinician will often ask about:
- which side bleeds
- how often and how long it lasts
- triggers (sleep, showers, exercise)
- medications/supplements
- family history and other bleeding symptoms
Some clinicians find a brief “nosebleed log” helpful—side, duration, what you were doing, and anything you tried.
Nasal exam (and what they’re looking for)
An exam may look for:
- dry spots and crusting
- a visible superficial vessel near the front of the nose
- signs of deviation or spurs
When imaging (like CT) is considered
CT isn’t needed for every nosebleed. It may be considered in more complex cases or when planning procedures.
*Specific details about side, frequency, and triggers can speed diagnosis and guide treatment.*
Treatment options if a deviated septum is contributing
First‑line: treat dryness and irritation
Even when deviation is present, clinicians usually start with:
- moisturizing and humidity measures
- reducing irritation/trauma
- managing allergies
- reviewing medication contributors with your prescribing team
This is also a useful “test”: if bleeding improves with moisture and habit changes, that’s strong evidence dryness/irritation was a major factor—whether or not a deviation exists.
Office‑based treatments for recurrent anterior bleeds
If a specific bleeding point is seen, options may include:
- cautery
- nasal packing in selected cases
When septoplasty enters the conversation
Septoplasty may be discussed when:
- bleeding is frequent/recurrent and other causes have been addressed
- the exam suggests the deviation or a spur is repeatedly drying/traumatizing tissue
- nasal obstruction symptoms significantly affect quality of life
For more detail, see: Can septoplasty help with chronic nosebleeds?: https://www.clearpathnasal.com/blog/can-septoplasty-help-with-chronic-nosebleeds
*Start simple; escalate to procedures if a specific bleeding site or structural issue keeps the problem going.*
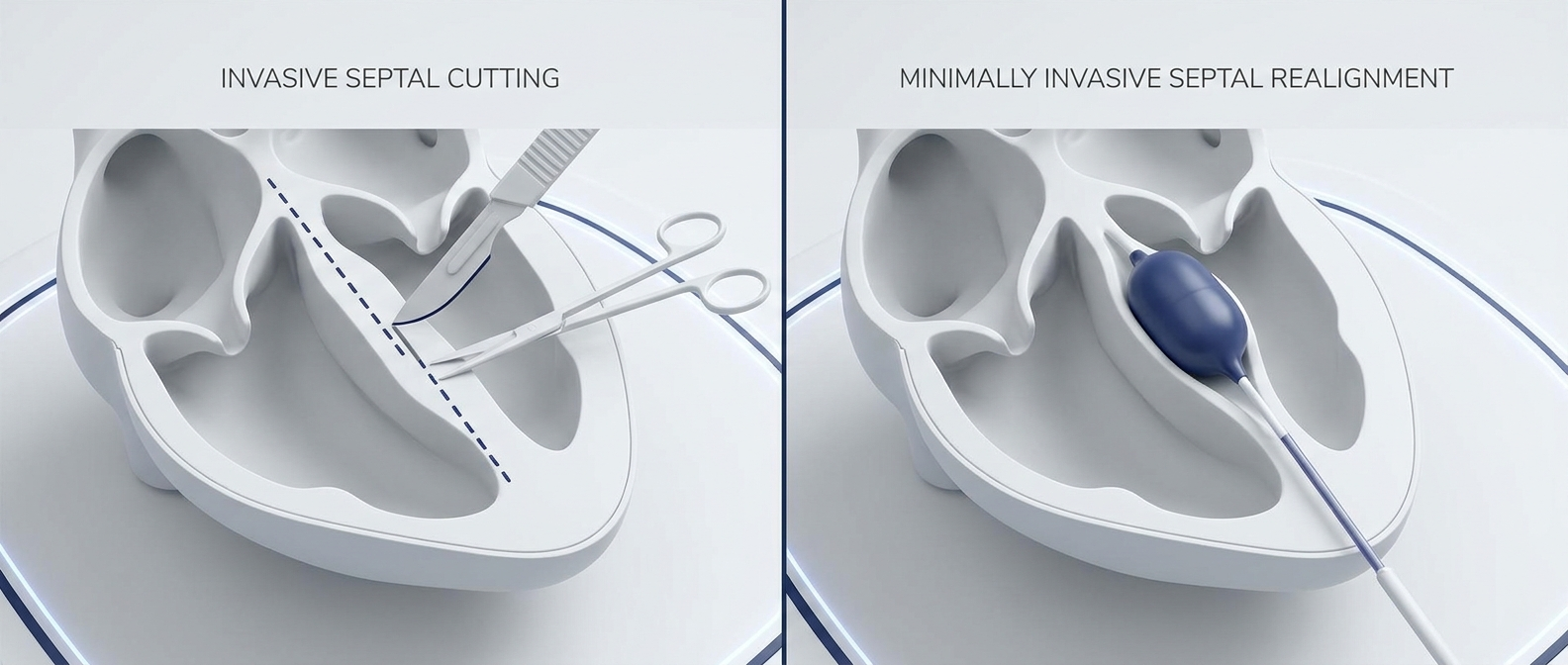
Minimally invasive approaches your ENT may discuss (including balloon‑assisted techniques)
What “minimally invasive” can mean for septal correction
In some patients, ENTs may discuss less invasive approaches designed to improve airflow and reduce irritation with less tissue disruption than traditional surgery. One option discussed in select cases is balloon‑assisted septoplasty, where a balloon is used to help reshape septal cartilage. ClearPath is one device that may be used in some balloon‑assisted septoplasty approaches. A clinician can determine whether a minimally invasive option is appropriate for a given patient.
Evidence snapshot (balloon‑assisted septoplasty cohort)
In one retrospective case series (Dillard et al., 2026, Rhinology Online) of 107 consecutive balloon‑assisted septoplasty cases, the authors reported no major complications in that cohort (including no septal perforation, hematoma, infection, or conversion to traditional septoplasty). In a subgroup with pre‑ and post‑operative CT scans, septal alignment improved at measured landmarks (reported as 22% improvement at the nasolacrimal duct and 45% at the point of maximal deviation). Patient‑reported symptoms (SNOT‑22) improved at one month among respondents (58.7 to 44.8; 23.8% reduction). As with all procedures, risks and outcomes vary by patient and setting.
To learn the basics, see: What is balloon septoplasty?: https://www.clearpathnasal.com/blog/what-is-balloon-septoplasty-a-minimally-invasive-option-for-deviated-septum
*Minimally invasive options exist for selected patients; your ENT can help decide if one fits your anatomy and goals.*
FAQs
Can a deviated septum cause nosebleeds?
Yes—deviated septum–related nosebleeds can happen when airflow changes dry and irritate the lining or when a spur causes repeated localized trauma. But dryness, irritation, and inflammation are still among the most common drivers overall.
Why do I only get nosebleeds on one side?
Often it’s a localized dry spot or fragile vessel. A deviation may contribute by making one side drier or more crust‑prone.
When is a nosebleed “too frequent”?
If you have recurrent nosebleeds—with or without a deviated septum—and bleeding keeps happening despite humidity/moisturizers, or it’s hard to stop or affecting your life, consider an evaluation.
Will septoplasty stop my nosebleeds?
Sometimes, but not always. Septoplasty is typically considered when the deviation/spur is clearly contributing and common triggers have been addressed first.
*Your pattern, exam findings, and response to conservative care help predict which treatments will work best.*
Takeaway + next step
If you’re repeatedly thinking “why does my nose bleed—deviated septum?”, the most practical answer is: it might be contributing, but it’s rarely the only factor.
- Nosebleeds often come from dryness and irritation.
- A deviated septum can increase risk by changing airflow, increasing crusting, and sometimes causing localized trauma.
- Because septal deviation is common, recurrent bleeding deserves a broader evaluation.
If nosebleeds are frequent, heavy, or keep returning, schedule an ENT exam to pinpoint the bleeding source and discuss next‑step options—including conservative care, office treatment, traditional septoplasty, or, for appropriate candidates, minimally invasive approaches.
*A focused evaluation can identify your main triggers and match you with the least invasive effective solution.*
This article is general information and not a substitute for medical care. If bleeding is heavy or won’t stop, seek urgent help.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.