

Why Do I Snore? The Deviated Septum Connection
If you’ve ever wondered, “why do I snore?”, you’re not alone. Snoring is common—and it’s rarely caused by a single factor. One often-missed contributor is your nose, especially if a deviated septum or other nasal blockage makes nasal breathing harder at night.
This guide connects the dots between deviated septum snoring, mouth breathing, and sleep quality—plus practical steps and treatment options (including when surgery may help and when it may not). The goal is realistic expectations: better airflow, improved sleep comfort, and a clearer plan if sleep apnea is part of the picture.
Snoring 101: What’s Actually Making the Sound?
The basics—vibration from partially blocked airflow
Snoring happens when airflow is partially blocked and soft tissues start to vibrate. The sound can come from:
- The soft palate and uvula
- The tongue base
- The throat walls
- The nasal passages (less common, but possible)
Snoring often gets worse when you’re:
- In deeper stages of sleep (muscles relax more)
- Sleeping on your back (gravity encourages the tongue and soft palate to shift backward)
Common snoring triggers (quick checklist)
Many people have a few triggers working together:
- Nasal congestion/obstruction
- Alcohol or sedatives close to bedtime
- Back sleeping
- Weight gain
- Allergies/colds
- Age-related airway changes
If your snoring fluctuates night-to-night, inflammation (like allergies) or sleep position may be a major driver—not just anatomy.
Bottom line: Snoring is a vibration problem made worse when airflow can’t move smoothly.

How Your Nose Can “Set Off” Snoring (Even If the Noise Is in Your Throat)
Nasal obstruction raises resistance—so you compensate by mouth-breathing
Your nose is designed to be the primary pathway for breathing during sleep. When the nose is blocked—due to a deviated septum, allergies, enlarged turbinates, or other causes—air faces more resistance. Many people then unconsciously switch to mouth breathing. That shift can change jaw and tongue position and make the throat more likely to narrow and vibrate, so mouth breathing snoring is often a downstream effect of an upstream nasal problem.
A common pattern: you fall asleep fine, wake up with a dry mouth, and your partner reports louder snoring on nights when your nose felt “plugged.” That’s a classic clue that nasal obstruction and snoring are traveling together.
A helpful analogy
Imagine breathing like sipping a drink through a straw. If the front end of the straw is pinched (your nose is obstructed), it takes more suction to pull air through. That extra “pull” can make the more flexible part of the airway (the throat) narrow and flutter. A 2022 systematic review suggests that nasal blockage can increase airway resistance and contribute to mouth breathing, which may worsen snoring and OSA-related breathing patterns [1].
Bottom line: When the nose is blocked, the throat can become the weak link that vibrates.

Deviated Septum: The “Crooked Wall” in the Middle of Your Nose
What a deviated septum is (and what it isn’t)
Your septum is the wall of cartilage and bone that separates your left and right nasal passages. When it’s deviated, one side may be narrower—sometimes both sides are affected depending on the shape. Many people have a mild deviation and feel fine. It becomes more relevant when it causes persistent nasal obstruction, especially at night—when tissues naturally swell a bit and you’re more sensitive to airflow resistance.
Symptoms that suggest your septum may be part of the problem
- Chronic one-sided nasal congestion (or one side that’s “always worse”)
- Difficulty breathing through your nose during exercise or sleep
- Waking with dry mouth (a sign of nighttime mouth breathing)
- Recurrent sinus pressure or a “stuffy” facial feeling
- Sleep that feels unrefreshing even after enough hours
For a deeper dive, see deviated septum and snoring: https://www.clearpathnasal.com/blog/deviated-septum-and-snoring-why-a-balloon-procedure-may-help
Bottom line: If your nose is consistently tight—especially on one side—it may be nudging you toward mouth breathing and snoring.

Snoring vs. Sleep Apnea: When a “Simple Snore” Might Be More Serious
Key differences (plain language)
- Snoring = sound from vibration due to partially blocked airflow.
- Obstructive sleep apnea (OSA) = repeated episodes of significant airflow reduction or pauses in breathing during sleep, often causing oxygen drops and brief awakenings.
Red flags that warrant a sleep evaluation
- Loud snoring plus choking/gasping or “snort-awakenings”
- Witnessed pauses in breathing
- Significant daytime sleepiness, brain fog, or morning headaches
- High blood pressure or elevated heart/cardiac risk factors
Where the septum fits in
Nasal obstruction can contribute to snoring and may worsen OSA-related breathing changes—but fixing the nose alone isn’t usually a complete OSA cure [1–3]. For more context, see deviated septum and sleep apnea: https://www.clearpathnasal.com/blog/deviated-septum-and-sleep-apnea-can-clearpath-improve-breathing-at-night
Bottom line: Snoring can be simple, but certain signs point to OSA—get checked if you notice them.

How Clinicians Figure Out Whether Your Nose Is Driving Your Snoring
At-home clues (before you book an appointment)
- Your snoring worsens during allergy season or with colds
- You wake with dry mouth or a sore throat (mouth breathing overnight)
- “Open nose” nights and “blocked nose” nights track with snoring intensity
If you’re unsure whether it’s structure or inflammation, this comparison may help: deviated septum vs allergies: https://www.clearpathnasal.com/blog/deviated-septum-vs-allergies-how-to-tell-the-difference
A quick 30-second “nose vs. throat” self-check
- If you breathe through your nose while awake, is one side consistently tight?
- Do you snore less when you can breathe clearly through your nose (after a shower, humidifier, saline rinse)?
- Do you wake up with dry mouth even when you sleep long enough?
- Does your snoring change noticeably with sleep position (back vs. side)?
In-office evaluation (what to expect at ENT)
- A symptom review (nasal breathing, sleep quality, snoring pattern)
- A nasal exam (sometimes with a small camera/endoscopy)
- Checking for turbinate enlargement, nasal valve collapse, polyps, or chronic swelling
- If apnea is suspected: a home sleep test or in-lab sleep study
Bottom line: Sorting out structural vs inflammatory causes usually points to the right first steps.
Treatment Options—Start Simple, Then Get Specific
Step 1: Reduce nasal inflammation and improve airflow (non-surgical)
- Saline rinses and/or humidification
- Allergy management (avoidance strategies and appropriate medications)
- Nasal steroid sprays (when indicated)
- Short-term decongestants (use cautiously to avoid rebound congestion)
Step 2: Mechanical and behavior strategies at night
- Side-sleeping or positional strategies
- Avoid alcohol/sedatives near bedtime (they relax airway muscles)
- If you have clear nasal blockage patterns, your ENT may discuss options aimed at improving nasal airflow
Step 3: If you have OSA—why nasal airflow still matters
Even when snoring is tied to sleep apnea, improving nasal breathing can still be valuable. Clinical guidelines support evaluating nasal obstruction in patients with OSA, and nasal surgery may be considered to improve symptoms and help patients tolerate standard sleep-apnea therapies rather than as a primary cure [3].
Bottom line: Calming nasal inflammation and improving airflow often reduce snoring burden—and can support broader sleep-apnea care.

Septoplasty for Snoring—What the Research Actually Shows (Realistic Expectations)
What septoplasty tends to improve (subjective benefits)
When a deviated septum is truly blocking airflow, septoplasty often helps appropriately selected patients feel better—especially nasal breathing and sleep-related symptoms. Studies commonly show improvements in subjective outcomes like sleepiness and perceived sleep quality, though results vary [1].
What septoplasty usually does not do by itself (OSA severity)
In a 2022 meta-analysis, the average reduction in apnea-hypopnea index (AHI) after isolated nasal surgery was small—about 4 events per hour—though results varied across studies [1]. Translation: you may breathe and sleep more comfortably, but a sleep study number may not change much from septoplasty alone if the main collapse point is the soft palate or tongue base.
When combining procedures matters (septum + turbinates)
In one 2014 study, septoplasty plus inferior turbinate reduction was associated with greater AHI improvement and higher treatment success than septoplasty alone in selected patients [2]. If your turbinates are enlarged, addressing them at the same time may be part of an effective plan.
Bottom line: Septoplasty can meaningfully improve nasal breathing and sleep symptoms, but it isn’t usually a stand-alone fix for OSA.
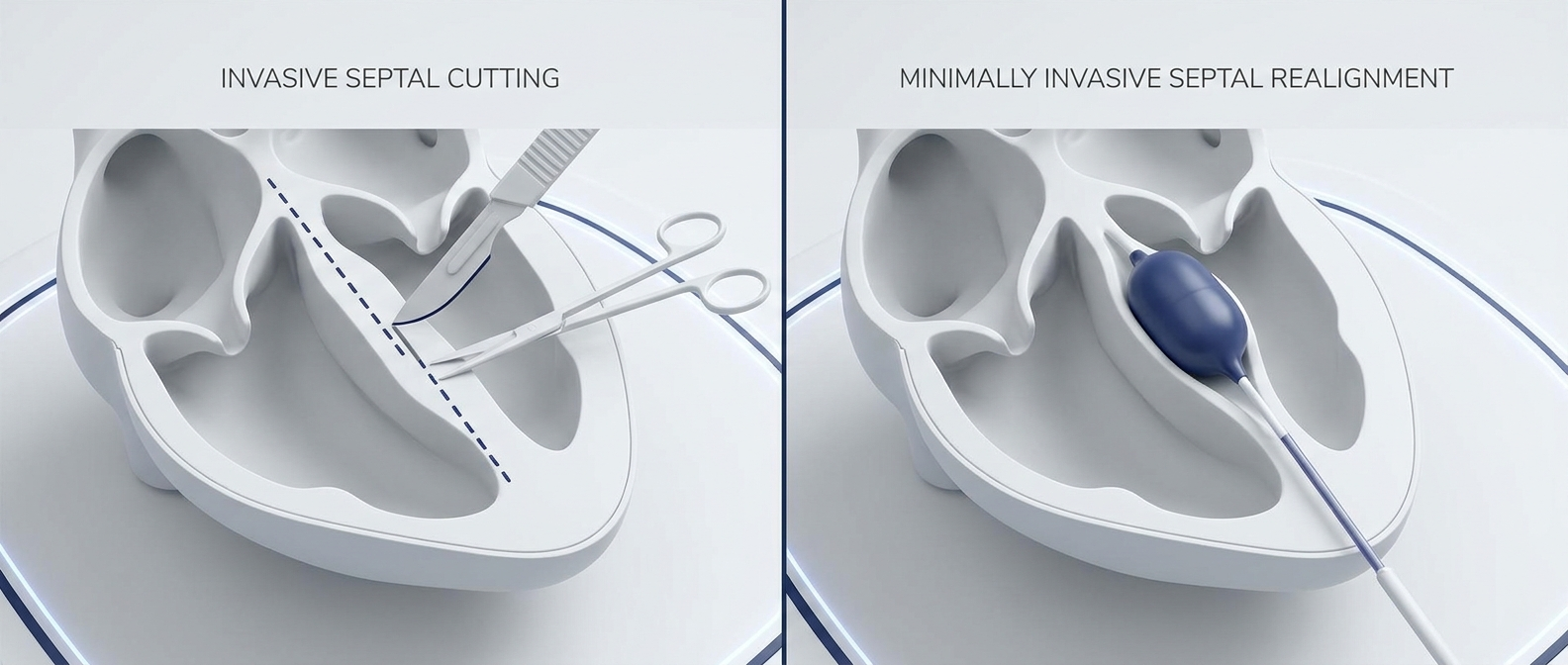
Minimally Invasive Options (And What “Balloon” Approaches Aim To Do)
Traditional septoplasty is a well-established option for improving nasal airflow in the right candidates. Some practices also offer minimally invasive, balloon-assisted techniques designed to support septal remodeling with less tissue disruption. ClearPath is described as a device used in a minimally invasive, balloon-assisted approach that may help support septal remodeling and improve nasal airflow in appropriate candidates. To understand the concept, see what is balloon septoplasty?: https://www.clearpathnasal.com/blog/what-is-balloon-septoplasty-a-minimally-invasive-option-for-deviated-septum
Bottom line: The right approach depends on your anatomy, goals, and exam findings—ask which option fits you best.
Are You a Good Candidate for Septoplasty (With or Without Turbinate Reduction)?
Good-fit signs
- Clear anatomic blockage plus persistent nasal obstruction
- Mouth breathing at night that seems tied to nasal blockage
- Snoring that correlates with “blocked-nose” nights
- Trouble tolerating standard sleep-related treatments primarily because your nose feels blocked [3]
Situations where septoplasty may not help much
- Snoring is mainly driven by tongue base/soft palate collapse
- There are no meaningful nasal obstruction symptoms
- Weight-related OSA is present without significant nasal blockage symptoms
When referral is reasonable
If snoring is bothersome and you also have clear symptoms of nasal blockage, a referral to an otolaryngologist for evaluation (including whether septoplasty ± turbinate treatment makes sense) is reasonable [3].
Bottom line: Matching the treatment to the true blockage points is key to better outcomes.
Questions To Ask an ENT (Quick Visit-Prep List)
Diagnosis clarity
- Is my obstruction from septal deviation, turbinates, nasal valve collapse, allergies—or a mix?
- Would you recommend turbinate reduction along with septoplasty?
Sleep-focused outcomes
- Should I get a sleep study to rule out sleep apnea?
- What changes should I realistically expect—snoring loudness, sleep quality, daytime sleepiness?
Recovery and risks
- What is the typical recovery timeline for the approach you recommend?
- What short-term effects are common (swelling, congestion, dryness)?
- What are the main risks, and how are they minimized?
- Am I a candidate for a minimally invasive, balloon-assisted septal approach, or is a traditional septoplasty a better fit for my anatomy?
Quick Recap—Why the Septum Connection Matters
- Nasal blockage (including a deviated septum) can increase resistance and contribute to mouth breathing, which may worsen snoring and OSA-related breathing patterns [1].
- Septoplasty often improves how people feel (breathing, sleep comfort, sleepiness), but by itself usually produces only a small average change in AHI [1].
- If turbinates are also enlarged, combining septoplasty with turbinate reduction may lead to better objective sleep-breathing outcomes in selected patients; nasal surgery is most often considered for symptom relief and to support tolerance of standard OSA treatments rather than as a stand-alone cure [2–3].
Bottom line: Treat the nose for comfort and support—treat the whole airway for OSA.
FAQ
Can a deviated septum cause snoring?
Yes. By creating nasal obstruction, a deviated septum can push you toward mouth breathing and increase airway vibration—making deviated septum snoring more likely, especially when you sleep on your back or during allergy/cold seasons. For more detail, see can a deviated septum cause snoring?: https://www.clearpathnasal.com/blog/deviated-septum-and-snoring-why-a-balloon-procedure-may-help
Why is my snoring worse when my nose is stuffed up?
A stuffed nose increases resistance to airflow and often triggers mouth breathing. That change in airflow and throat position can increase vibration, which is why nasal obstruction and snoring commonly worsen together [1].
Will septoplasty cure sleep apnea?
Usually not by itself. Septoplasty can improve nasal breathing and sleep symptoms, but studies show only a small average improvement in AHI after isolated nasal surgery [1]. It may still play an important supporting role in an overall sleep-apnea treatment plan [3].
Does turbinate reduction help snoring more than septoplasty alone?
It can, when enlarged turbinates are a major source of blockage. In one 2014 study, septoplasty combined with inferior turbinate reduction was associated with greater AHI improvement and higher treatment success than septoplasty alone in selected patients [2].
When should I get a sleep study for snoring?
Consider a sleep study if you have loud snoring plus choking/gasping, witnessed pauses in breathing, significant daytime sleepiness, morning headaches, or cardiovascular risk factors. If you’re not sure, start with an ENT or primary care visit to review symptoms and next steps.
References
1. Isolated Nasal Surgery in Obstructive Sleep Apnea: A Systematic Review (2022). https://pmc.ncbi.nlm.nih.gov/articles/PMC9688553/
2. Effects of Septoplasty With or Without Inferior Turbinate Reduction on OSA (2014). https://pmc.ncbi.nlm.nih.gov/articles/PMC4211927/
3. Clinical Practice Guideline for Nasal Surgery in OSA (2022). http://e-ceo.org/journal/view.php?doi=10.21053/ceo.2022.01361
Next Step
If your snoring is bothersome and you also have persistent nasal blockage (especially one-sided congestion or nightly mouth breathing), consider scheduling an evaluation with a local ENT. Discuss your snoring goals, ask whether septoplasty ± turbinate reduction makes sense for you, and—if you prefer minimally invasive options—ask whether a balloon-assisted septal approach is appropriate for your anatomy.
Disclaimer
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.