

What Is the Nasolacrimal (Tear) Duct?
Introduction — Why the “Tear Duct” Matters
Tears don’t simply disappear after they wash over your eyes. Under normal circumstances, they drain through a small plumbing system at the inner corner of the eyelids, and ultimately empty into the nose. That’s why your nose can run when you cry: the extra fluid has to go somewhere, and the nose is the exit route.
When something disrupts that drainage—especially a nasolacrimal duct obstruction (NLDO)—you may notice persistent watery eyes, mucus-like discharge, or crusting. This is especially common in babies, but it can affect adults too. In this article you’ll learn what the nasolacrimal duct (sometimes called the “tear duct,” and less commonly the “nasal lacrimal duct”) is, how tear drainage works, why blockages happen, how clinicians diagnose them, and the step-by-step treatment options. Sources: StatPearls (Anatomy) and StatPearls (NLDO) via NCBI Bookshelf.
• In short: tears drain into the nose; when that drainage is blocked, eyes water and discharge can build up. •
What Is the Nasolacrimal (Tear) Duct?
The nasolacrimal duct is a drainage channel that carries tears from the lacrimal sac (near the inner corner of the eye) down into the nose—specifically into the inferior nasal meatus (a space along the side wall of the nasal cavity). If you like analogies, think of it as the final downspout that takes fluid from the collection area near the eye and directs it into the nose. Sources: StatPearls—Anatomy, Head and Neck: Eye Nasolacrimal (2023); Kenhub (2024).
Nasolacrimal duct vs. “tear duct” — are they the same?
In everyday conversation, people often say “tear duct” to describe the entire tear drainage system. Anatomically, the system includes several parts (small openings, tiny channels, a sac, and then the duct). The nasolacrimal duct is one specific segment—an important one—because it’s the final pathway that delivers tears into the nose. A practical way to picture it: if the puncta and canaliculi are the drains and pipes, the lacrimal sac is the collection tank, and the nasolacrimal duct is the main line that empties into the nasal cavity.
Where does it drain?
Tears travel from the eye area into the nose. When you cry, the system can be overwhelmed, and more fluid ends up in the nasal cavity—leading to sniffles and a runny nose. Many clinicians explain it simply: “Your eyes and nose are connected by drainage—so big tears can become a runny nose.” Sources: StatPearls (2023); Kenhub (2024).
• In short: the nasolacrimal duct is the last channel that takes tears into the nose. •
Tear Drainage Anatomy (Step-by-Step)
If you’re trying to make sense of watering eyes, it helps to understand the normal route tears are supposed to take. When any part of that route narrows or blocks, tears can spill over the eyelid instead of draining efficiently.
The normal tear outflow pathway
Here’s the usual pathway, step-by-step: - Puncta (tiny openings on the eyelid margins near the inner corner) - Canaliculi (small channels that carry tears inward) - Lacrimal sac (a small collection reservoir) - Nasolacrimal duct (the drainage “pipe” down into the nose) - Inferior nasal meatus (where tears enter the nasal cavity). Sources: StatPearls—Anatomy (2023); Kenhub (2024).
What the lacrimal sac does
The lacrimal sac acts like a small holding area where tears collect before moving down the nasolacrimal duct. If drainage is blocked farther downstream, the sac can become overfilled. Patients (or parents) often notice this as persistent tearing plus discharge that returns soon after wiping—because the reservoir keeps refilling. Stagnant fluid can also set the stage for irritation or infection, which is why clinicians pay close attention to redness, swelling, and tenderness near the inner corner of the eye.
Why nasal anatomy can matter for tear drainage
Because the tear drainage system opens inside the nose, nasal structure and swelling can sometimes affect symptoms or influence how certain procedures are performed. For example, if the nasal lining is inflamed or the anatomy is tight, it may change how clinicians evaluate the nasal end of the drainage pathway. For a quick refresher on spaces and structures inside the nose, see ClearPath’s overview of nasal anatomy: https://www.clearpathnasal.com/blog/deviated-septum-causes-understanding-your-nasal-anatomy.
ClearPath is also the name of a proprietary nasal balloon device used in certain procedures. Understanding where key structures sit inside the nasal cavity can help patients follow discussions about endoscopic evaluation and treatment planning.
• In short: tears drain through a series of tiny structures into the nose, so nasal anatomy can influence symptoms and procedures. •

How the Nasolacrimal Duct Develops (And Why Babies Commonly Have Blockage)
Embryology in plain language: canalization
During fetal development, the tear drainage pathway forms and then opens up (a process called canalization). Sometimes, the lowest end of the system doesn’t fully open by birth, so tears can’t drain efficiently. Parents often describe it as “one eye that always looks watery,” even when the baby isn’t upset. Source: StatPearls—Nasolacrimal Duct Obstruction (2023).
The valve of Hasner and distal blockage (most common)
The most common site of congenital blockage is near the bottom of the drainage pathway—close to where it enters the nose—often described as the area of the valve of Hasner. In plain terms: the exit door into the nose is the spot most likely to still be partially closed in early infancy. Source: StatPearls—NLDO (2023).
How common is congenital NLDO, and when does it get better?
Symptoms consistent with congenital NLDO are reported in about 6–20% of newborns, and many cases improve without a procedure by 6–12 months of age. That timeline is why clinicians often recommend conservative care first when the baby is otherwise well and there are no signs of infection. Source: StatPearls—NLDO (2023).
• In short: most infant tear-duct blockages are at the nasal exit and often resolve on their own by the first year. •

Common Problems of the Tear Duct (NLDO and Beyond)
Congenital nasolacrimal duct obstruction (babies)
In infants, NLDO often shows up as one persistently watery eye, sometimes with discharge. A common pattern is that the eye waters more in wind, cold air, or during an upper respiratory infection—times when tearing can increase and the drainage system has to work harder. Many improve with conservative care and time. Sources: American Academy of Ophthalmology (AAO, 2015); StatPearls—NLDO (2023).
Acquired obstruction (older children/adults)
In older children and adults, obstruction can develop later due to inflammation, scarring, narrowing of the drainage pathway, or structural changes that interfere with normal flow. This can lead to ongoing tearing (epiphora) and recurring discharge. Adults may report annoyance with constant tearing on one side, blurred vision from tears pooling, or irritation from frequent wiping. Source: StatPearls—NLDO (2023).
• In short: babies often have temporary congenital blockage, while adults can develop obstruction later from inflammation or structural change. •
Symptoms — What a Blocked Tear Duct Feels/Looks Like
Key symptoms
Common signs of a drainage problem include: - Watery eyes (epiphora) not related to emotion - Mucus or mucopurulent discharge - Crusting on the lashes, often worse after sleep. Sources: AAO (2015); StatPearls—NLDO (2023).
When it’s more than “just watering”
Seek medical guidance sooner if symptoms suggest infection or significant inflammation, such as: - Redness and swelling near the inner corner of the eye - Increasing tenderness or pain - Fever (especially in infants). Source: StatPearls—NLDO (2023).
• In short: persistent tearing with discharge is common, but pain, redness, or fever are red flags that need prompt care. •

Possible Complications (When You Should Seek Care Quickly)
Dacryocystitis (infection of the lacrimal sac)
When tears can’t drain, stagnant fluid can contribute to bacterial growth, sometimes causing dacryocystitis (infection of the lacrimal sac). Typical features include tender swelling near the inner corner, redness, and discharge. Clinicians take this seriously because infections around the eye can worsen quickly without appropriate care. Source: StatPearls—NLDO (2023).
Dacryocystocele in infants (rare, but important)
A dacryocystocele is a cyst-like swelling related to blockage in the tear drainage pathway. It’s uncommon, but clinicians take it seriously—particularly in newborns—because severe cases can be associated with more significant infection risks (including orbital cellulitis or systemic illness). Sources: StatPearls—NLDO (2023); AAO (2015).
“Red flags” checklist (patient-friendly)
Seek urgent evaluation if you notice: - Fever in an infant - Rapidly increasing swelling or redness near the inner corner - Severe eyelid swelling or the eye appears pushed forward - Trouble breathing or feeding if nasal blockage is suspected (infants). Source: StatPearls—NLDO (2023).
• In short: painful swelling, fever, or rapidly worsening redness near the inner corner of the eye merits urgent medical care. •
How Clinicians Diagnose Nasolacrimal Duct Problems
History and eye exam basics
Diagnosis usually starts with questions and an eye exam: when tearing began (since birth vs later), whether one or both eyes are involved, the pattern of discharge, and signs of irritation. Clinicians may look for an increased tear meniscus (a visible “pool” of tears along the lower lid). In clinic, you might hear a simple summary like: “The eye is making tears, but they’re not draining the way they should.” Source: StatPearls—NLDO (2023).
Dye Disappearance Test (what it is and what it shows)
One common in-office assessment is the dye disappearance test. A small amount of dye is placed in the eye, and the clinician checks after a short time to see whether it drained normally. If dye remains, it can support suspicion of an outflow problem—especially when it matches the history and exam findings. Source: StatPearls—NLDO (2023).
When imaging or specialist testing is considered
If symptoms are persistent, recurrent, complicated, or atypical, additional testing or specialist evaluation may be recommended. Sometimes this includes evaluating the nasal side of the drainage pathway. For background on how clinicians visualize structures inside the nose, you may find this overview of endoscopic nasal procedures helpful: https://www.clearpathnasal.com/blog/endoscopic-septoplasty-vs-open-surgery-which-is-better. Sources: AAO (2015); StatPearls—NLDO (2023).
• In short: diagnosis usually involves history, exam, and simple tests, with endoscopic or imaging studies when cases are persistent or atypical. •

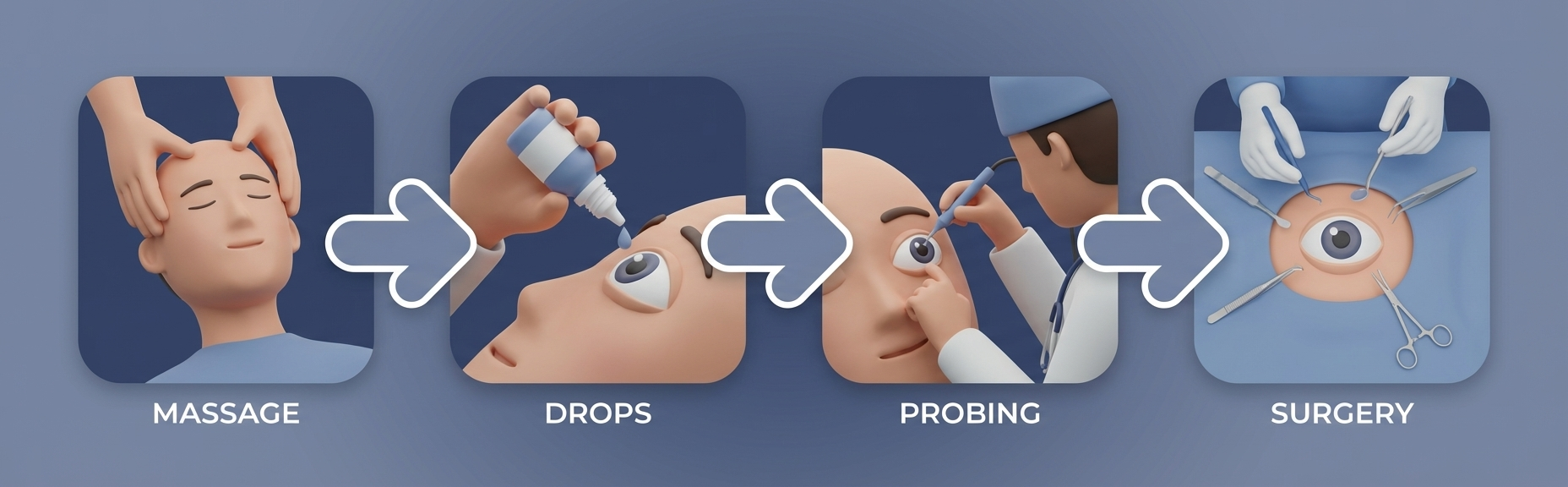
Treatment Options (Stepwise, Starting With the Simplest)
First-line care for infants: massage and hygiene
Many infants improve with time plus conservative measures. Clinicians commonly recommend gentle lacrimal sac massage (pressure applied in a way intended to help move fluid through the drainage pathway) along with cleaning away discharge as advised. Warm compresses may also be suggested in some cases. Because so many cases resolve naturally, watchful waiting is often appropriate in otherwise well infants. The goal is comfort and cleanliness while the duct finishes opening. Sources: AAO (2015); StatPearls—NLDO (2023).
Antibiotic drops/ointment — when they’re used
Antibiotic drops or ointment may be prescribed when discharge suggests infection or significant bacterial overgrowth. However, antibiotics generally help manage discharge and infection—they do not open the blockage by themselves. Overuse or inappropriate use can contribute to antimicrobial resistance; always use them only as directed by a clinician. Sources: AAO (2015); StatPearls—NLDO (2023).
Probing (common next step when it doesn’t resolve)
If symptoms persist, a common next step is probing, where a clinician gently passes a thin instrument through the tear drainage pathway to open the obstruction. Timing and setting depend on the child’s age and the specifics of the case, but success rates are generally high in infants. Sources: AAO (2015); StatPearls—NLDO (2023).
Surgery for persistent or complex cases
When obstruction persists or is more complex—especially in adults—surgical options may be considered. One well-known approach is dacryocystorhinostomy (DCR), which creates a new drainage pathway into the nose. Because the nose is part of the final drainage destination for tears, nasal anatomy and nasal procedures sometimes come up during planning. For readers curious about procedure settings, here’s a patient-friendly look at what to expect with minimally invasive, office-based nasal procedures: https://www.clearpathnasal.com/blog/what-to-expect-during-an-office-based-balloon-septoplasty. And if you want to understand how nasal balloon technology works in general, this step-by-step explainer may help: https://www.clearpathnasal.com/blog/how-the-clearpath-nasal-balloon-works-a-step-by-step-guide. Balloon-based dilation devices are sometimes used to treat nasal obstructions that affect airflow or contribute to symptoms and may be an alternative or complement to more traditional surgical approaches, depending on individual anatomy and diagnosis.
• In short: many infant cases resolve with conservative care; persistent blockage can often be treated with probing or, in complex cases, surgery that creates or optimizes nasal drainage. •
When to See an Ophthalmologist (and When to Refer Urgently)
Appropriate watchful waiting vs. evaluation
For infants with mild tearing and discharge but no concerning signs, conservative care and monitoring are often reasonable—especially early on, since many cases improve by 6–12 months. If symptoms persist beyond the expected window, keep recurring, or are worsening, an ophthalmology evaluation is appropriate. Sources: AAO (2015); StatPearls—NLDO (2023).
Urgent evaluation triggers
Seek urgent care for suspected infection (dacryocystitis), suspected dacryocystocele, fever, or rapidly increasing swelling/redness around the inner corner of the eye. Source: StatPearls—NLDO (2023).
• In short: monitor mild infant tearing early on, but seek prompt evaluation for persistence, worsening symptoms, or any red flags. •
FAQs (Patient-Friendly)
Why does my baby have one watery eye?
Congenital NLDO often affects one side. A blockage near the valve of Hasner can prevent normal drainage, leading to persistent watering and sometimes discharge. Source: StatPearls—NLDO (2023).
Can a blocked tear duct cause “pink eye”?
A blocked system can cause discharge and crusting that look similar to conjunctivitis. It can also occur alongside true conjunctivitis. A clinician can help determine whether symptoms are from infection on the eye surface, a drainage problem, or both. Sources: AAO (2015); StatPearls—NLDO (2023).
Is watery eye always a blocked tear duct?
Not always. Allergies, irritation, and dry eye can trigger reflex tearing. Still, if tearing is persistent (especially with discharge), evaluating the tear drainage pathway—including the nasolacrimal duct—is often part of the workup. Source: StatPearls—NLDO (2023).
Will it go away on its own?
Many infants improve naturally, often by 6–12 months, particularly with conservative measures. Persistent cases can be treated effectively with procedures such as probing. Source: StatPearls—NLDO (2023).
Key Takeaways (Quick Summary)
- The nasolacrimal duct is the final channel that drains tears into the nose (inferior nasal meatus). - A common issue in infants is congenital distal blockage near the valve of Hasner, leading to NLDO. - Symptoms often include watery eyes, discharge, and crusting; infection is an important “red flag.” - Many infant cases resolve with time and conservative care; persistent cases may benefit from probing, and complex cases may need surgery such as DCR. Sources: StatPearls—Anatomy (2023); StatPearls—NLDO (2023); AAO (2015).
Call to action (CTA)
If you or your child has ongoing tearing or recurrent discharge, consider scheduling an evaluation with an eye-care specialist. You can also discuss with your healthcare provider whether nasal anatomy contributes to your symptoms and explore possible treatment options, including balloon dilation devices.
Sources
- StatPearls/NCBI Bookshelf. Anatomy, Head and Neck: Eye Nasolacrimal (2023). https://www.ncbi.nlm.nih.gov/books/NBK482213/ - StatPearls/NCBI Bookshelf. Nasolacrimal Duct Obstruction (NLDO) (2023). https://www.ncbi.nlm.nih.gov/books/NBK532873/ - American Academy of Ophthalmology (AAO). Nasolacrimal Duct Obstruction in Children (2015). https://www.aao.org/education/disease-review/nasolacrimal-duct-obstruction-4 - Kenhub. Nasolacrimal duct (2024). https://www.kenhub.com/en/library/anatomy/nasolacrimal-duct
Disclaimer
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.