

The Role of Turbinates in Nasal Obstruction Explained
If you feel like you “can’t get air through your nose,” it’s easy to blame allergies—or assume you just have a stubborn cold. But one of the most common (and most overlooked) contributors is inside your nose all the time: your nasal turbinates.
Understanding the role of turbinates in nasal obstruction can help you make sense of why congestion becomes chronic, why one side may feel worse than the other, and why some people don’t get lasting relief from sprays alone. The key takeaway: turbinates are essential for healthy breathing, but when they enlarge, they can narrow the nasal airway and significantly reduce airflow. That can affect sleep, exercise, and daily comfort. (See references [1], [3].)
You’ll often hear patients describe this as, “I’m not sick—I just feel blocked,” or “I can breathe through my mouth, but my nose never feels clear.” That experience is common when the issue is primarily swelling and narrowed space rather than a lot of mucus.
The Role of Turbinates in Nasal Obstruction (Quick Overview)
Turbinates are curved structures along the sidewalls of the nasal cavity. They’re not “extra tissue”—they’re part of the nose’s built-in air-processing system. They warm, humidify, and filter inhaled air and help regulate airflow. (References [1], [3].)
Problems start when turbinates become persistently swollen or enlarged (often due to inflammation, rhinitis, or compensation for a crooked septum). In that situation, the role of turbinates in nasal obstruction becomes very noticeable: less nasal space means more resistance, which can feel like constant congestion—even without visible mucus. (References [1], [2].)
A helpful way to picture it: your nose is more like a climate-controlled air system than an open pipe. If the “air-conditioning fins” (turbinates) swell, air has to squeeze by—so breathing feels harder even if you’re not producing much discharge.
Summary: Healthy turbinates fine-tune airflow; swollen turbinates narrow the path and raise resistance.
What Are Nasal Turbinates?
Where turbinates are located (and why “inferior turbinates” matter most)
Most people have three turbinates on each side of the nose:
- Inferior turbinates
- Middle turbinates
- Superior turbinates
While all three affect airflow, the inferior turbinates sit lowest and take up a meaningful portion of the nasal airway. Because of their size and location, inferior turbinates are most often involved in chronic nasal obstruction. (References [1], [3].)
If your main complaint is day-to-day blockage (especially when lying down), your clinician often pays close attention to the inferior turbinates because that’s where small changes in swelling can translate into a big change in airflow.
What turbinates do for your breathing (more than “extra tissue”)
Turbinates help your nose do three big jobs:
1. Conditioning inhaled air: warming and humidifying air before it reaches the lungs
2. Filtering: trapping particles in mucus and moving them out over time
3. Regulating airflow: shaping airflow patterns and nasal resistance
Turbinates contain mucosa and vascular (blood vessel–rich) tissue that can swell and de-swell as part of the normal “nasal cycle,” where one side may be slightly more open than the other at different times. This is usually normal—until swelling becomes persistent or excessive. (References [1], [2], [3].)
Clinicians sometimes explain it like this: “Your turbinates are meant to be dynamic.” They’re supposed to adjust. The problem isn’t that they move—it’s when they stay enlarged and stop “resetting.”
Summary: Turbinates are dynamic, not static; trouble starts when they stay enlarged instead of cycling back down.

How Turbinates Cause Nasal Obstruction
What is turbinate hypertrophy?
Turbinate hypertrophy means enlargement of the turbinates—most commonly the inferior turbinates. It’s frequently associated with chronic nasal blockage and can be a major reason patients feel they can’t breathe well through their nose. (References [1], [4].)
People often describe it as:
- “My nose feels blocked, but I’m not really blowing mucus out.”
- “I can breathe for a little while after a spray, then it closes again.”
That pattern often points to swelling of the turbinate lining rather than a temporary infection.
The “plumbing” explanation: narrowing the airway increases resistance
Think of your nasal airway like a hallway. If the walls swell inward, the walkway narrows. With turbinates, enlargement reduces available space for airflow. Even small decreases in airway diameter can noticeably increase resistance.
Another everyday analogy: pinching a drinking straw just a little can make it feel much harder to pull liquid through. In the nose, that “pinch” can come from swollen turbinate tissue rather than something you can blow out.
Importantly, turbinate enlargement is often driven more by swollen submucosal/vascular tissue than by bony overgrowth—meaning inflammation and blood flow changes can play a big role in how blocked you feel day to day. (References [1], [2].)
Common symptoms patients notice
When turbinate size and swelling are driving symptoms, patients often report:
- Persistent stuffiness (sometimes worse at night)
- Mouth breathing and dry mouth
- Reduced exercise tolerance (you feel “air hungry” sooner)
- Snoring or sleep disruption
- A feeling of pressure/fullness (and sometimes headache), especially if obstruction is significant
These symptoms can overlap with other nasal obstruction causes, which is why a focused evaluation matters. (References [1], [4].)
A practical example: some people notice they can breathe “okay” while upright during the day, but once they lie down, congestion ramps up and they wake up with a dry mouth. That pattern commonly fits turbinate swelling and nasal resistance.
Summary: Even a small increase in turbinate size can create a big jump in airflow resistance—and very real daily symptoms.

Why Do Turbinates Enlarge? (Most Common Causes)
Allergic rhinitis (seasonal or year-round allergies)
Allergies can trigger ongoing inflammation inside the nose. Over time, that inflammation can lead to chronic swelling of the turbinate lining and symptoms that look like “constant congestion.” (References [1], [3].)
You might notice an allergy pattern like: worse symptoms during pollen seasons, around pets, or after dust exposure—plus sneezing, itching, or watery discharge. Even when those classic allergy symptoms fade, the swelling can linger.
Non-allergic (vasomotor) rhinitis
Not all nasal swelling is allergy-based. Non-allergic rhinitis can be triggered by things like:
- Temperature or humidity changes
- Smoke or strong odors
- Pollution/irritants
- Spicy foods
This can cause turbinate swelling without the classic allergy mechanism. (References [1], [3].)
A common clue is inconsistency: you may feel congested after a hot shower, walking into cold air, or being near fragrance—yet allergy testing (if done) may not match your symptom pattern.
Chronic hypertrophic rhinitis / long-term inflammation
When inflammation becomes persistent, the lining of the nose can remain chronically thickened and reactive. This can contribute to ongoing turbinate enlargement and a long-term blocked sensation. (References [1], [3].)
In day-to-day life, this may look like “baseline congestion” that never fully clears—then flares with colds, travel, seasonal changes, or irritants.
Compensatory turbinate hypertrophy from a deviated septum
A deviated septum means the wall between the nostrils is off-center. When one side is narrowed structurally, the opposite side may develop compensatory turbinate hypertrophy over time—essentially the turbinate enlarges on the roomier side, which can still leave you feeling obstructed overall. (References [1], [3].)
If a deviated septum is involved, here’s how it contributes to obstruction: Deviated Septum Explained: Symptoms, Causes, and Modern Treatment Options: https://www.clearpathnasal.com/blog/deviated-septum-explained-symptoms-causes-and-modern-treatment-options
This is also why treating only one issue (just the septum or just the turbinates) may leave symptoms behind for some patients.
Summary: Pinpointing the main driver—allergy, irritants, or structure—helps you choose the right fix.

Turbinates vs. Deviated Septum vs. Allergies—How to Tell What’s Driving Your Blockage
Clues it may be mostly turbinate swelling
- Symptoms fluctuate with triggers (allergens, irritants, weather changes)
- Congestion varies side-to-side over hours
- Partial/temporary improvement with appropriate medical therapy (like anti-inflammatory nasal sprays used correctly)
A patient-style way this sounds is: “It’s never the same side for long,” or “Some days are fine, then the next day I’m completely blocked.”
Clues it may be more structural (septum + compensatory turbinate hypertrophy)
- One side feels consistently worse for months or years
- A long history of obstruction that doesn’t respond much to typical allergy care
- You notice blockage even when you’re otherwise well (no seasonal pattern)
This often comes across as: “It’s always the left,” or “I’ve had this since I got hit in the nose years ago.”
Why you can have both (and many patients do)
Many patients have “stacked” obstruction: a structural narrowing (like a deviated septum) plus inflammatory swelling (like turbinate hypertrophy). That’s why a personalized plan matters. (References [1], [3].)
Allergies can mimic structural blockage—here’s how to separate them: Deviated Septum vs Allergies: How to Tell the Difference: https://www.clearpathnasal.com/blog/deviated-septum-vs-allergies-how-to-tell-the-difference
Summary: Track your patterns—fluctuating swelling points to turbinates; constant one-sided blockage points to structure.
How ENTs Evaluate Turbinates and Nasal Obstruction
Office history + symptom review (what your clinician will ask)
A clinician will usually ask about:
- Seasonality and triggers
- Medication history (what you’ve tried and for how long)
- Sleep quality, snoring, mouth breathing
- Whether one side is always worse
- Environmental exposures (smoke/irritants)
If you can, bring specifics (even a quick note on your phone): what makes symptoms worse, what helps, and which treatments you’ve tried consistently versus occasionally.
Physical exam and nasal endoscopy (what it looks for)
A nasal exam (often including endoscopy) can assess:
- Turbinate size and swelling patterns
- Septal deviation
- Signs of inflammation
- Other contributors to blockage
This helps clarify the role of turbinates in nasal obstruction versus other structural or inflammatory causes. (Reference [1].)
When imaging (CT) is used
CT imaging isn’t required for everyone, but it may be used when:
- Anatomy is complex
- Symptoms are severe or persistent
- Surgical planning is being considered
(Reference [1].)
Summary: A targeted history, nasal exam, and—if needed—CT usually reveal why airflow feels limited.
Non-Surgical Treatments for Turbinate Hypertrophy (First-Line Options)
Many cases of turbinate swelling improve with consistent, targeted medical care.
Daily saline rinses (supportive care)
Saline rinses can help wash out irritants, reduce crusting, and thin mucus. They don’t “shrink bone,” but they can reduce the inflammatory load in the nose.
For people exposed to dust, pollen, or workplace irritants, this can be a simple “reset” at the end of the day—especially during flare seasons.
Nasal steroid sprays (inflammation control)
For allergic rhinitis and many non-allergic inflammatory conditions, nasal steroid sprays are often a foundation therapy to reduce swelling over time (not instantly). Nasal steroids usually require consistent daily use over weeks to months for maximal effect; technique and patience matter. (Reference [1].)
A common reason they “don’t work” is timing and technique—these sprays typically need consistent daily use, and many patients feel meaningful improvement after days to weeks rather than minutes.
Allergy-focused medications when appropriate
Depending on symptoms and clinician guidance, this may include:
- Non-sedating antihistamines
- Environmental control strategies (reducing exposure)
If allergies are a big driver, controlling the trigger load can reduce how often turbinates “stay swollen” in the first place.
Non-allergic rhinitis options
For non-allergic triggers, treatment often focuses on:
- Trigger reduction
- Clinician-directed nasal sprays based on symptom pattern
This can be especially helpful when your symptoms reliably track with irritants, strong scents, weather shifts, or certain foods.
A brief caution on overusing decongestant sprays
Short-term decongestant sprays can give fast relief, but using them too frequently or for too many days in a row can lead to rebound congestion. If you feel “stuck” needing a spray, it’s worth discussing alternatives with a clinician.
Summary: Consistency is key—daily, correct use of anti-inflammatory care often beats “as-needed” quick fixes.

When Turbinate Reduction Surgery Is Considered
Signs medical therapy isn’t enough
Turbinate reduction surgery may be considered when:
- Obstruction persists despite appropriate medical therapy
- Symptoms significantly affect sleep, exercise, or daily function
- The turbinates remain consistently enlarged on exam
(References [1], [4].)
Many ENTs frame it simply: if you’ve truly addressed inflammation and triggers and still can’t breathe, it may be time to talk about a structural solution—ideally one that preserves turbinate function.
Common turbinate reduction approaches (high-level, patient-friendly)
There are different ways to reduce enlarged turbinates, but many modern approaches aim to be mucosa-sparing—meaning they reduce volume while preserving the lining needed for humidifying and filtering.
Depending on anatomy, an ENT may discuss options such as:
- Submucosal reduction techniques
- Office- or OR-based volume reduction approaches
- Outfracture (repositioning) in selected cases
The goal is improved airflow without eliminating turbinate function. (References [1], [3].)
Why preserving turbinate function matters
Turbinates help condition and regulate airflow. Over-reducing them can lead to unwanted dryness and airflow discomfort in some cases—rarely, patients may develop a constellation of symptoms sometimes referred to as empty nose syndrome. That’s why careful, function-preserving planning is important. (References [1], [3].)
Summary: The best surgical plans create space while protecting the nose’s natural climate-control system.

If a Deviated Septum Is the Main Driver: Septoplasty Options (Including Minimally Invasive Techniques)
Why septal deviation can worsen turbinate-related obstruction
A deviated septum reduces space on one side and may contribute to compensatory turbinate hypertrophy on the other. If both issues are present, addressing only the septum or only the turbinates may not fully relieve symptoms. (References [1], [3].)
This is also why two people with “the same” deviation can feel very different—because turbinate swelling, inflammation, and nasal cycle variability can amplify the sensation of blockage.
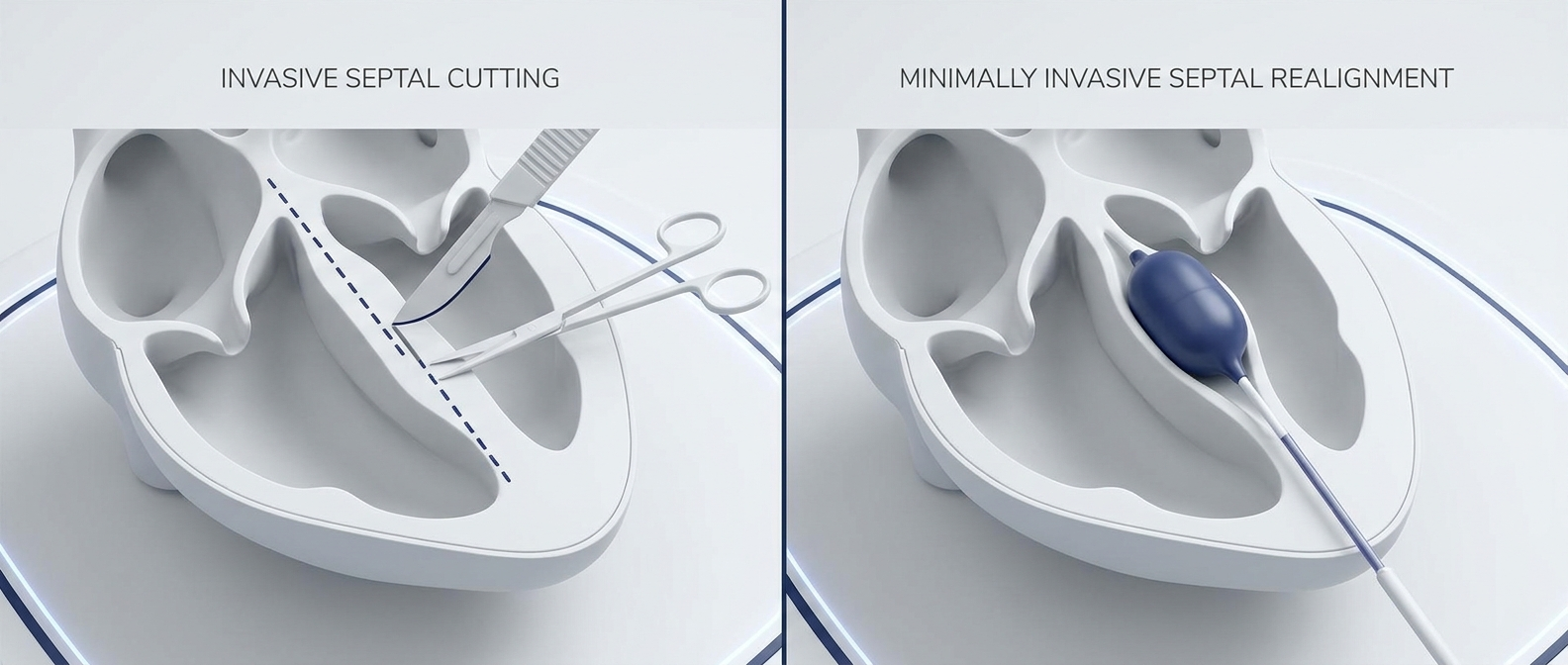
Balloon-assisted endoscopic septoplasty (overview for patients)
For patients whose obstruction is primarily structural, septoplasty may be recommended. Some practices also offer balloon-assisted endoscopic septoplasty, which can be performed using the ClearPath Nasal Balloon, a device designed to help reshape and reposition deviated septal cartilage with endoscopic guidance.
In the right candidates, this approach may be an alternative to more traditional septoplasty techniques, potentially reducing the amount of tissue disruption compared with standard methods—depending on anatomy and surgical goals. If you’re exploring options, you can ask your local ENT whether you’re a candidate for balloon-assisted endoscopic septoplasty and whether ClearPath is appropriate for your situation.
Learn what balloon septoplasty is and who it may help: What Is Balloon Septoplasty? A Minimally Invasive Option for Deviated Septum: https://www.clearpathnasal.com/blog/what-is-balloon-septoplasty-a-minimally-invasive-option-for-deviated-septum
For patients with septal deviation, minimally invasive options may help—here’s a step-by-step explanation: How the ClearPath Nasal Balloon Works: A Step-by-Step Guide: https://www.clearpathnasal.com/blog/how-the-clearpath-nasal-balloon-works-a-step-by-step-guide
Example outcomes reported with the ClearPath Nasal Balloon technique (brief, evidence-based)
What one study found (retrospective case series):
- 107 cases: no major intraoperative or postoperative complications observed in the series (as reported), such as septal perforation, hematoma, or synechia
- Symptoms: SNOT-22 decreased by about 24% at 1 month, with improvements noted in congestion, headache/facial pressure, and sleep quality
- Imaging subset (n=23): CT showed about 45% mean improvement at maximal deviation and 22% at the nasolacrimal duct (p=0.005)
- The authors also described potential efficiency benefits related to less flap elevation, packing, and suturing in their technique
(Reference [5].)
When septoplasty is combined with turbinate reduction
It’s common for ENTs to evaluate the septum and turbinates together. In patients with both septal deviation and turbinate hypertrophy, combining septoplasty with turbinate reduction can be considered to address both structural narrowing and inflammatory/compensatory enlargement when indicated. (References [1], [3].)
Summary: When structure is the main problem, septoplasty—sometimes with turbinate reduction—can restore balance to both sides.
Recovery Expectations and When to Follow Up
What congestion after treatment can mean
After medical treatment changes—or after procedures—temporary swelling during healing can still cause congestion. Improvement is often gradual as inflammation settles and tissues recover.
A realistic timeline helps reduce anxiety: many patients notice “ups and downs” early on, then steadier improvement as the lining calms and nasal airflow normalizes.
Here are practical septoplasty recovery tips and a realistic timeline: Septoplasty Recovery Tips: Getting Back to Normal Faster: https://www.clearpathnasal.com/blog/septoplasty-recovery-tips-getting-back-to-normal-faster
When to call your clinician
Seek medical guidance if you develop:
- Heavy bleeding
- Fever
- Worsening pain that doesn’t respond to the expected plan
- New, severe one-sided symptoms
Summary: Expect some variability early; most patients see steadier progress as healing continues.
FAQ (SEO-Friendly)
Can turbinates grow back after reduction?
Modern turbine reduction techniques are typically tissue-sparing and do not remove all turbinate structures. Turbinates don’t “grow back” as new bone, but the remaining tissue can become swollen again if the underlying driver (allergies, non-allergic rhinitis, irritant exposure) persists. Some patients benefit from ongoing anti-inflammatory care even after a reduction, and a minority may need touch-up treatment over time depending on technique and triggers.
Are enlarged turbinates dangerous, or just annoying?
Enlarged turbinates are usually not dangerous, but they can meaningfully affect quality of life—sleep, exercise, and daytime energy. Persistent obstruction is worth evaluating because it may also coexist with other treatable issues.
Do allergies cause turbinate hypertrophy permanently?
Allergies can drive chronic swelling, and long-term inflammation can make tissues more persistently reactive. Many patients improve with consistent allergy management; others may still have significant blockage and consider procedural options.
What’s the difference between turbinate hypertrophy and nasal polyps?
Turbinate hypertrophy is enlargement of normal nasal structures (turbinates). Nasal polyps are inflammatory growths that can form in the nasal lining and sinuses. They can both cause obstruction, but they are different conditions and are managed differently.
If I fix my septum, will my turbinates shrink?
Sometimes compensatory turbinate hypertrophy improves after septal correction, but not always. Many patients benefit from an individualized plan that considers whether turbinate reduction is needed at the same time as septal work.
Call to Action (Next Step)
If nasal blockage is affecting your sleep, workouts, or daily comfort, consider scheduling an evaluation with a qualified ENT. Ask whether your symptoms fit turbinate hypertrophy, a deviated septum, or (commonly) a combination—and whether options like balloon-assisted endoscopic septoplasty (including ClearPath) could be appropriate for you compared with traditional approaches.
Medical disclaimer: This article is for general educational purposes only and does not provide medical advice. Diagnosis and treatment depend on your symptoms, exam findings, and medical history. For personalized guidance, consult a licensed clinician.
Disclaimer: This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
References
1. NCBI Bookshelf. Turbinate Hypertrophy (overview and related nasal obstruction concepts). https://www.ncbi.nlm.nih.gov/books/NBK546636/
2. PubMed Central (PMC). Turbinate hypertrophy / submucosal tissue contribution and obstruction mechanisms. https://pmc.ncbi.nlm.nih.gov/articles/PMC11147595/
3. ScienceDirect Topics. Turbinate: anatomy and function summary. https://www.sciencedirect.com/topics/medicine-and-dentistry/turbinate
4. Dr. Hester ENT. What is Turbinate Hypertrophy and How is it Treated? https://www.drhesterent.com/what-is-turbinate-hypertrophy-and-how-is-it-treated/
5. Dillard JD, Koudouovoh C, Lee V, et al. Outcomes of force-directed balloon-assisted endoscopic septoplasty: a retrospective analysis with a new technique and device. Rhinology Online. 2026;9:18–23. http://doi.org/10.4193/RHINOL/25.018
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.