

The Role of the Vomer Bone in Nasal Blockage
If you’ve ever felt like your nose is “blocked deep inside”—especially on one side—you may wonder whether it’s allergies, swollen turbinates, or something structural. One often-overlooked structural contributor is the posterior part of the nasal septum, where a thin bone called the vomer helps form the divider between your nasal passages.
This article explains how vomer anatomy can relate to nasal obstruction in the back of the nose, how ear, nose, and throat specialists (ENTs) evaluate the posterior septum, and what treatments—including septoplasty and selected minimally invasive approaches—may help.

What the vomer bone is (and where it sits in your nose)
The nasal septum has cartilage and bone—here’s the simple breakdown
Think of the nasal septum as the wall separating the left and right nasal passages. Some parts are flexible, and some are rigid:
- Cartilage (front): the more flexible portion closer to the nostrils
- Perpendicular plate of the ethmoid (upper bone): a bony part higher in the septum
- Vomer (posteroinferior bone): a thin bone forming the posterior-inferior part of the septum
This matters because the back of the nose is a narrower “hallway” to begin with. When the posterior septum is crooked—especially if the bony parts are involved—it can reduce airflow in a meaningful way (Nasal Septal Deviation: A Comprehensive Narrative Review, 2022: https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/).
For a quick foundation on nasal structure, see understanding your nasal anatomy: https://www.clearpathnasal.com/blog/deviated-septum-causes-understanding-your-nasal-anatomy
Bottom line: the vomer is normal anatomy, but its position in the posterior septum can affect how easily air moves through the back of the nose.

Why the vomer matters for airflow (especially in the back of the nose)
The vomer helps define the shape of the posterior septum and can influence airflow in the posterior nasal passage. That’s why some people with a mainly back-of-the-nose deviation feel significantly obstructed even if the front of the septum doesn’t look dramatically off-center.
A simple analogy: if the front doorframe looks straight but the hallway narrows sharply near the back, you can still feel “stuck” moving through the space. In nose terms, posterior septal deviation involving the vomer can feel “deeper” than the usual stuffy-nose sensation (2022 narrative review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/).
If your congestion feels deep and toward the back, the posterior septum may be part of the reason.
Can the vomer bone cause nasal blockage?
The short answer: it can contribute—usually as part of a deviated bony septum
Most medical discussions don’t isolate the vomer alone; they discuss the bony septum (the vomer plus the perpendicular plate). When the posterior bony septum deviates, it can narrow the airway and contribute to nasal obstruction related to posterior septal deviation (2022 narrative review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/).
In practice, the vomer is part of a unit with other bony structures, and their combined position can influence airflow.
What “posterior septal deviation” can feel like
Patients often describe a posterior deviation using location-based language—more about “where” than “how intense,” for example: “It feels blocked behind my nostril, not at the entrance.”
Common descriptions include:
- One-sided congestion that doesn’t alternate sides
- A sensation of blockage behind the nostrils
- Trouble breathing through the nose during exercise
- Mouth-breathing or sleep disruption (snoring can occur but is nonspecific)
- Feeling blocked even after trying typical over-the-counter remedies
For symptom-focused steps you can consider, see what to do next for chronic nasal congestion: https://www.clearpathnasal.com/blog/deviated-septum-and-chronic-nasal-congestion-what-to-do-next
If symptoms localize “deeper” on one side and don’t respond to usual measures, a posterior deviation could be contributing.
Why vomer-specific answers are hard to find (the evidence gap)
Most studies evaluate:
- Overall deviation patterns (front and back), and/or
- Outcomes of correcting the whole septum
As a result, conclusions about the vomer’s independent role are usually indirect, not perfectly isolated (2022 narrative review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/).
Evidence generally addresses the entire septum, so vomer-only effects are difficult to separate out.
Common causes of vomer-related narrowing (and what’s rare)
Most common: part of a typical deviated septum
Many people have some degree of septal deviation. When the deviation involves the bony portion, it may be described as:
- Bony septal deviation
- Posterior septal deviation
- Deviation affecting the posterior nasal septum
Because the vomer sits back and low, posterior deviations can be harder to appreciate without a detailed exam. In some cases, they’re missed on a quick look with a nasal speculum and become clearer with nasal endoscopy or imaging (2022 narrative review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/).
Rare: isolated congenital vomer defects
True isolated vomer abnormalities (like congenital defects or partial absence) are uncommon and are mostly described in case reports rather than large studies (Congenital defect of the vomer bone: A rare cause of septal perforation, 2006: https://www.sciencedirect.com/science/article/abs/pii/S1871404806000955).
For most patients, posterior blockage is part of a broader septal deviation pattern rather than a rare isolated vomer issue.
How ENTs determine whether the posterior bony septum is part of the problem

The exam tools that matter (in plain language)
A good evaluation usually starts with your story and a focused nasal exam. Many ENTs think in two categories: inflammation (swelling) and structure (shape). A visit typically includes:
- History: duration, one-sided vs alternating, triggers (seasonal vs constant), impact on sleep/exercise
- Nasal endoscopy: a small camera exam that lets an ENT see deeper structures
- Structural check: septum position (front and back), turbinate size, nasal valve stability
- Inflammation check: signs of rhinitis or chronic swelling
The aim is to confirm what’s narrowing the airway—soft tissue swelling, septal shape, or both—because treatments differ.

When imaging (CT) can help
A CT scan isn’t necessary for everyone, but it can be useful when symptoms persist, the exam suggests deeper structural narrowing, or sinus disease is suspected. CT may show:
- The shape and location of a posterior bony deviation
- How much the airway is narrowed at specific points
- Other contributors like turbinate hypertrophy or sinus inflammation
(2022 narrative review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/)
Other issues that can mimic a “vomer problem”
Before assuming a bone is the cause, consider common look-alikes:
- Allergic or non-allergic rhinitis
- Inferior turbinate enlargement
- Nasal valve collapse
- Chronic sinusitis
If you’re trying to tease apart inflammation vs structure, this article can help: deviated septum vs allergies—how to tell the difference: https://www.clearpathnasal.com/blog/deviated-septum-vs-allergies-how-to-tell-the-difference
An in-person exam helps determine whether obstruction is driven by swelling, structure, or both.

Treatment overview—what actually helps if the posterior bony septum is deviated
Medical therapy can help swelling, but it won’t straighten bone
First-line care often targets inflammation:
- Saline rinses
- Nasal steroid sprays
- Allergy management (when relevant)
These can reduce swelling and improve airflow, but they do not change the shape of a bony septal deviation. If symptoms are mainly structural—such as posterior septal deviation involving the vomer—medical therapy may help somewhat but often doesn’t fully resolve the problem.
Septoplasty: how surgery addresses posterior bony deviation (including the vomer)
Septoplasty for nasal blockage aims to improve airflow by reshaping or removing parts of the septum that narrow the nasal passage. When deviation is posterior and bony, surgeons may address the bony septum, which can include reshaping or resecting portions of the vomer as part of the overall repair (The State of the Art in Septoplasty: A Review of the Latest Achievements: https://pmc.ncbi.nlm.nih.gov/articles/PMC12964075/).
What research shows overall: septoplasty generally improves obstruction from septal deviation
Across multiple studies and reviews, septoplasty is generally associated with improvement in nasal obstruction symptoms when septal deviation is a true driver of blockage. Most evidence supports septoplasty for septal deviation broadly; it rarely isolates the vomer alone as the single variable (Sources: 2022 narrative review https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/ and septoplasty review https://pmc.ncbi.nlm.nih.gov/articles/PMC12964075/).
For a side-by-side look at options and considerations, see ClearPath vs traditional septoplasty—recovery, safety, and results: https://www.clearpathnasal.com/blog/clearpath-vs-traditional-septoplasty-recovery-safety-results
Medical therapy treats swelling; septoplasty addresses shape. The right approach depends on what’s driving your obstruction.
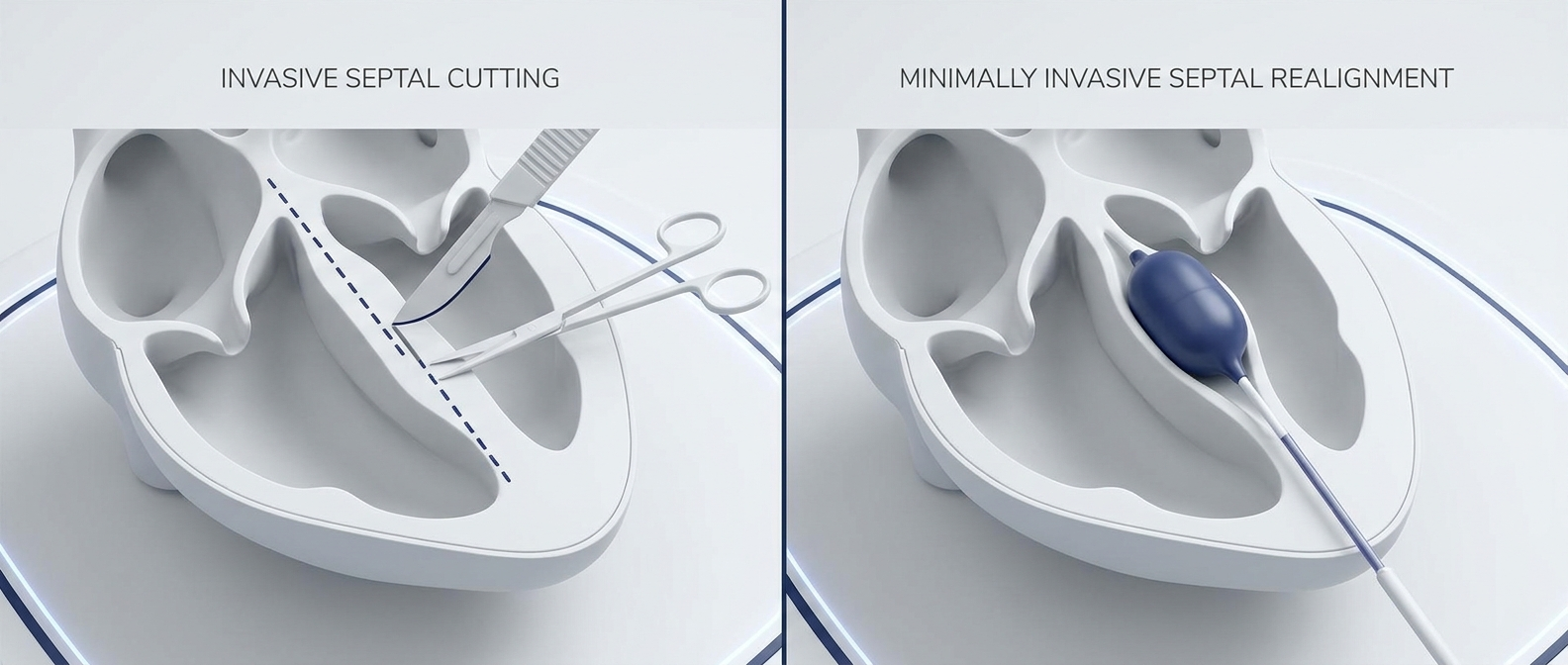
Minimally invasive septoplasty and posterior septal alignment (where the data is heading)
What a CNB-assisted septoplasty study reported (study-specific outcomes)
A retrospective review reported outcomes from 107 consecutive cases using a CNB-assisted approach. In a subgroup of 23 patients who had both pre- and post-operative CT scans, septal alignment symmetry improved by:
- 22% at the nasolacrimal duct
- 45% at the point of maximal deviation
In this study, the authors reported no major complications, including no septal perforation, hematoma, mucosal injury, infection, or conversion. For symptom outcomes, the subgroup with SNOT-22 data showed improvement from 58.7 to 44.8 at one month (a 23.8% reduction), with the largest improvements in congestion, facial pressure/headache, and sleep quality.
Source: Dillard J, Koudouovoh C, Lee V, et al. Rhinology Online. 2026;9:18–23. doi:10.4193/RHINOL/25.018
What this does—and doesn’t—suggest about the vomer specifically
These findings suggest that improving septal alignment, including posterior areas, can be associated with symptom improvement in selected patients. However, this does not prove a vomer-only cause-and-effect relationship, because posterior bony structures are typically evaluated and treated as part of the overall septum (context: 2022 narrative review https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/).
Early reports are encouraging for alignment-focused techniques, but broader, longer-term evidence is still developing.
When to talk to an ENT (and what to ask)
Signs you may have structural (not just inflammatory) blockage
Consider an evaluation if you notice:
- Long-standing, mostly one-sided obstruction
- Minimal improvement with sprays or allergy treatment
- Breathing difficulty during sleep or exertion
- A persistent “deep” blockage consistent with possible posterior septal deviation
Questions you can bring to the visit
- Is my deviation mainly cartilage, bone, or both?
- Is the posterior septum (including the vomer) narrowing my airway?
- Would septoplasty involve work on the bony septum?
- Am I a candidate for a traditional or minimally invasive septoplasty approach?
If you have persistent one-sided nasal obstruction, consider discussing your symptoms and treatment options with an ENT, including whether a posterior septal deviation may be contributing and which approaches may be appropriate.
An ENT can help clarify what’s driving your symptoms and which treatments align with your findings and preferences.
Key takeaways (patient-friendly summary)
- The vomer is a normal bone—but its position can matter for breathing. The vomer forms the back-bottom of the septum and can influence airflow in the posterior nasal passage. That’s why posterior obstruction can feel “deeper” than typical congestion.
- Most vomer-related blockage happens as part of a deviated septum. Isolated vomer defects are rare; symptoms more often reflect a combined cartilage and/or bony septal deviation (2022 review: https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/).
- Correcting septal deviation (including posterior bony parts) often improves symptoms. When a deviation is the main driver of obstruction, septoplasty is generally associated with symptom improvement, though vomer-only conclusions remain limited (https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/ and https://pmc.ncbi.nlm.nih.gov/articles/PMC12964075/).
FAQ
Can a deviated vomer cause one-sided congestion?
It can contribute, usually as part of a posterior nasal septum deviation. Many people describe a deep, persistent one-sided blockage when the posterior bony septum narrows airflow.
Will sprays fix a bony septal deviation?
Sprays can reduce swelling around the obstruction, but they do not straighten bone. If the main issue is structural (a bony septal deviation), symptoms may persist.
Does septoplasty change the vomer bone?
When the deviation involves the posterior bony septum, septoplasty may include reshaping or removing parts of the bony septum, which can include vomer portions, when clinically indicated (Septoplasty review: https://pmc.ncbi.nlm.nih.gov/articles/PMC12964075/).
Are congenital vomer defects common?
No. They are uncommon and largely described in case reports rather than large studies (2006 case report: https://www.sciencedirect.com/science/article/abs/pii/S1871404806000955).
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.