

The “Leap Frog” Technique: Moving the Septum Segment by Segment
If you’ve been researching deviated septum treatment, you may have run into the phrase “leap frog technique septum” and wondered what it means. The confusion is understandable: “leapfrog” can sound like an official surgical method for moving the septum in steps, but that’s not how the term is most commonly used in published nasal surgery literature.
This article breaks down what “leapfrog” usually refers to, what people often mean when they describe “moving the septum segment by segment,” and how modern septal realignment approaches—including balloon-assisted septoplasty with the ClearPath device—are being evaluated with objective imaging and patient symptom scores.
Why Patients Hear “Leap Frog” in Nose Surgery (and Get Confused)
The problem: “Leap frog” isn’t a standard septoplasty term. In everyday conversations (and online), surgical terms can drift. Patients may see “leapfrog” used to describe step-by-step correction of a crooked septum—especially in discussions of minimally invasive septoplasty.
Key clarification: I could not identify a universally accepted, formally named “leap frog technique septum” in standard septoplasty nomenclature. Instead, “leapfrog” has a more specific meaning in published nasal reconstruction (more on that below), while “segment-by-segment correction” is better understood as a concept many surgeons use: addressing areas of deviation in a planned sequence.
A helpful analogy: if your septum is like a slightly warped bookshelf divider, you don’t always fix the whole shelf with one push. You identify the spots where it bows into the airway, correct one area, then re-check whether the rest still needs adjustment.

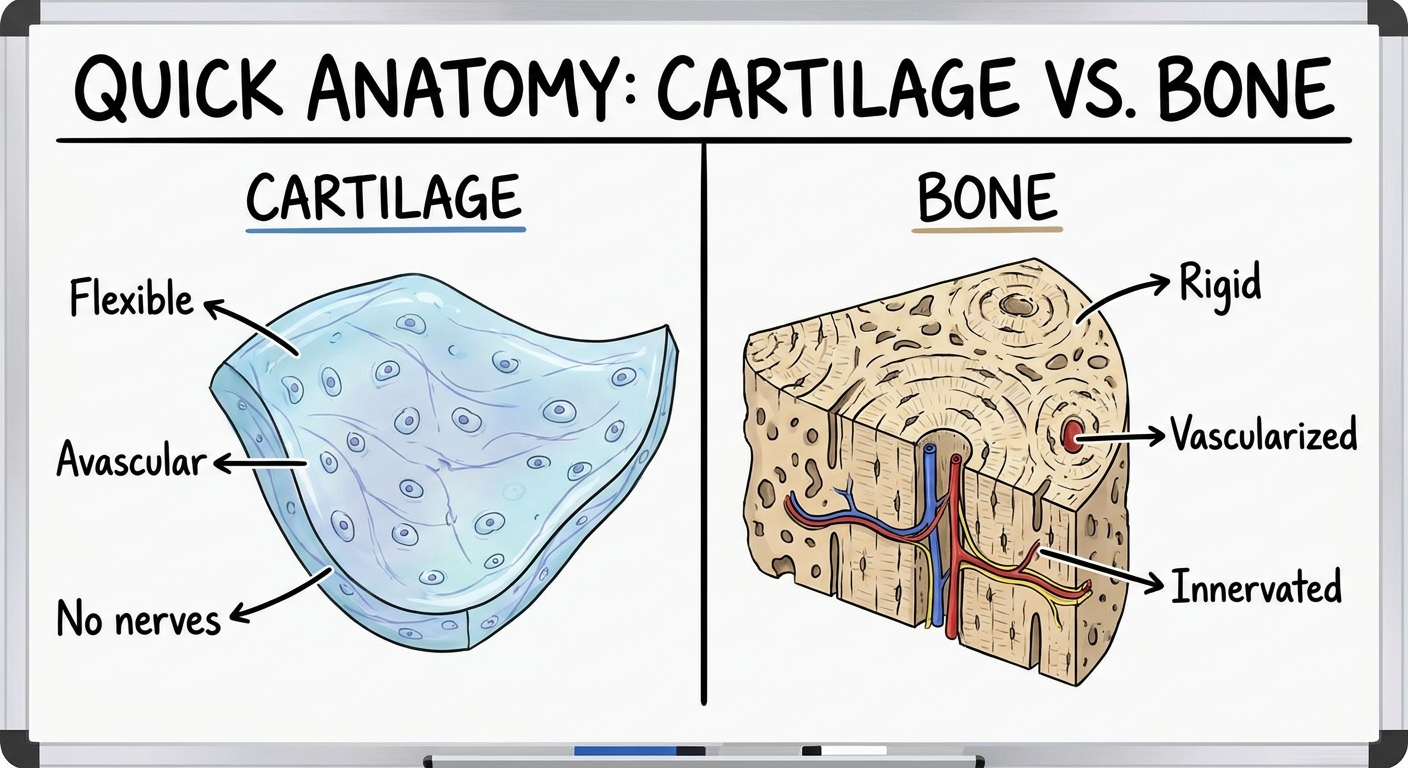
Quick anatomy refresher (in plain language)
The nasal septum is the wall in the middle of your nose that separates the left and right nasal passages. It’s made of cartilage toward the front (flexible but supportive) and bone toward the back (firmer).
A septum can deviate in different ways: a localized kink, a longer S-shaped bend involving multiple areas, or a deviation that affects nearby structures such as the nasal valve region.
When airflow is blocked, symptoms often include nasal obstruction, congestion, mouth breathing, sleep disruption, and pressure or headaches for some people. The goal of septal correction is nasal obstruction relief while preserving the support structures that help the nose function.
In short: “Leapfrog” in septoplasty is usually informal language for a sequential, targeted correction strategy—not a single, standardized maneuver.
The Recognized “Leapfrog” Term in Nasal Surgery: The Alar Leapfrog Technique
In the medical literature, the clearest “leapfrog” term is the Alar Leapfrog technique, described for cleft lip nasal reconstruction—not for standard deviated septum treatment. “Alar” refers to the outer/lower part of the nose around the nostril rim. In cleft reconstruction, surgeons often need to restore symmetry and support where the cartilage and soft tissue developed differently.
Citation: Pigott RW, 1985; PubMed PMID: 3905172. https://pubmed.ncbi.nlm.nih.gov/3905172/
How it works (simple explanation): alar cartilage is repositioned to improve projection and symmetry. The “leapfrogging” idea refers to moving cartilage onto or against sturdier supporting structures to create a more stable shape.
One way to picture it: rather than trying to stretch a weak structure to stand up on its own, you anchor it onto something more stable—so the final position holds.
Citations: PubMed PMID: 3905172; ScienceDirect (S0094129820316448). https://www.sciencedirect.com/science/article/pii/S0094129820316448
The septum’s role in Alar Leapfrog is foundation, not the moving part. The septum acts like a stable structure the alar cartilage is positioned against—not something being moved segment by segment.
Bottom line: In published usage, “leapfrog” most often refers to alar cartilage repositioning in cleft reconstruction, with the septum serving as support.
So What Could “Moving the Septum Segment by Segment” Mean in Plain English?
Many septal deviations are not a single smooth curve. They can have multiple high points—front versus back, cartilage versus bone, or a combination. That’s why your surgeon may talk about correcting the septum in a sequence: address one area, reassess straightness and airflow, then adjust the next. For a deeper primer, see understanding septal displacement: https://www.clearpathnasal.com/blog/understanding-septal-displacement
A common real-world example: a patient might feel blocked mainly on the left. On exam, the biggest pinch-point could be more forward (cartilage), while another deviation sits further back (bone). A segmental approach prioritizes what’s functionally limiting airflow.
Why segmental correction matters: preserve supportive tissue that helps the nose keep its shape and function; avoid unnecessary removal of septal material; focus correction where breathing is most restricted.
What patients often mean: “Straighten the front part first, then work backward.” Clinically: “Correct the main deviation, re-check the airway, then decide what else needs fine-tuning.” The underlying idea is sequential problem-solving—rather than a single named maneuver.
In essence: segment-by-segment is a practical way to describe planned, stepwise correction tailored to where the septum blocks airflow most.
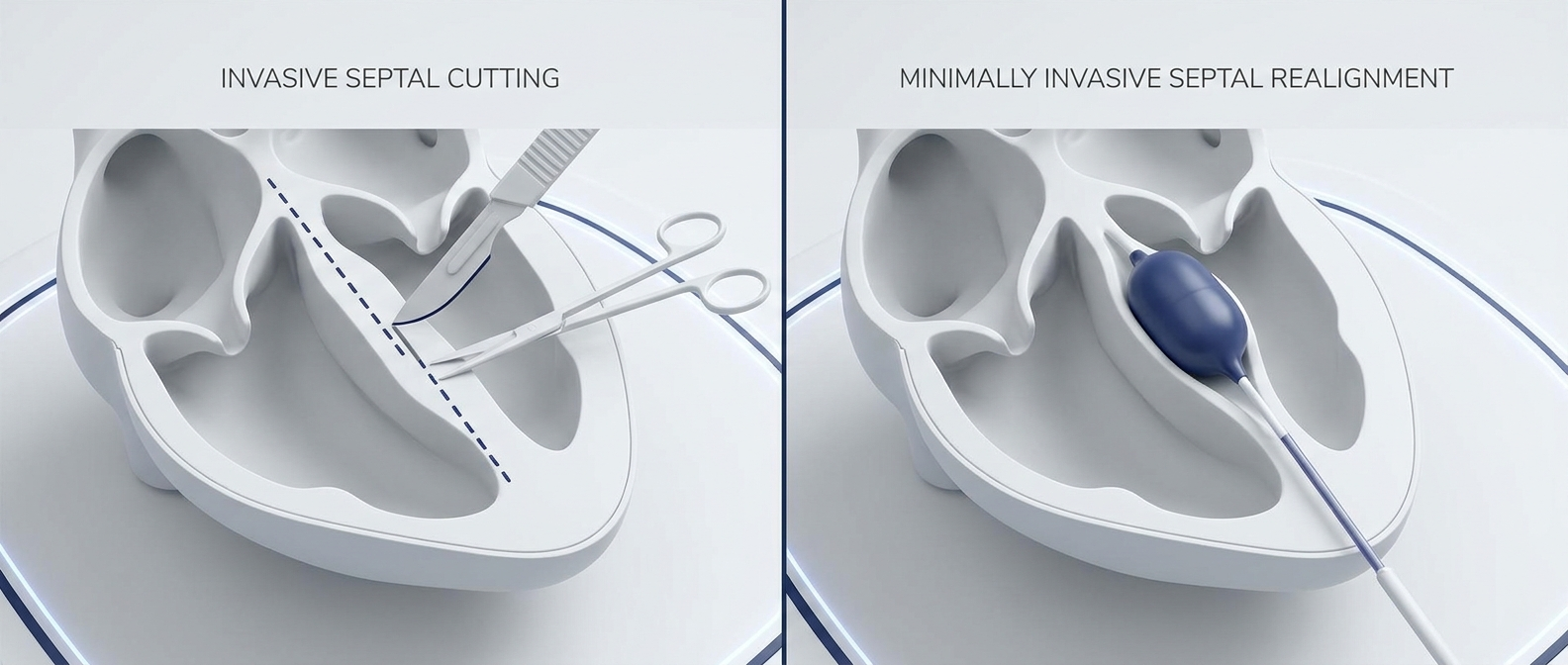
A Modern Example of Targeted Septal Realignment: Balloon-Assisted Septoplasty Outcomes
Modern approaches to septal realignment can be both controlled and measurable. One example is balloon-assisted septoplasty performed with the ClearPath device, designed to help reshape septal deviations in a targeted way. Basics: https://www.clearpathnasal.com/blog/what-is-balloon-assisted-septoplasty
ClearPath is described here as one possible approach discussed by the authors. Suitability depends on your anatomy, symptoms, and your clinician’s judgment.

What a large 2026 cohort showed (scale + credibility)
A 2026 retrospective review reported outcomes from 107 consecutive balloon-assisted septoplasty cases: 23 patients had pre- and post-operative CT scans (objective measurement), and 43 patients completed SNOT-22 symptom surveys (patient-reported outcomes).
Citation: Dillard J, Koudouovoh C, Lee V, et al. Rhinology Online. 2026;9:18–23. doi:10.4193/RHINOL/25.018
CT results: measurable improvements in alignment
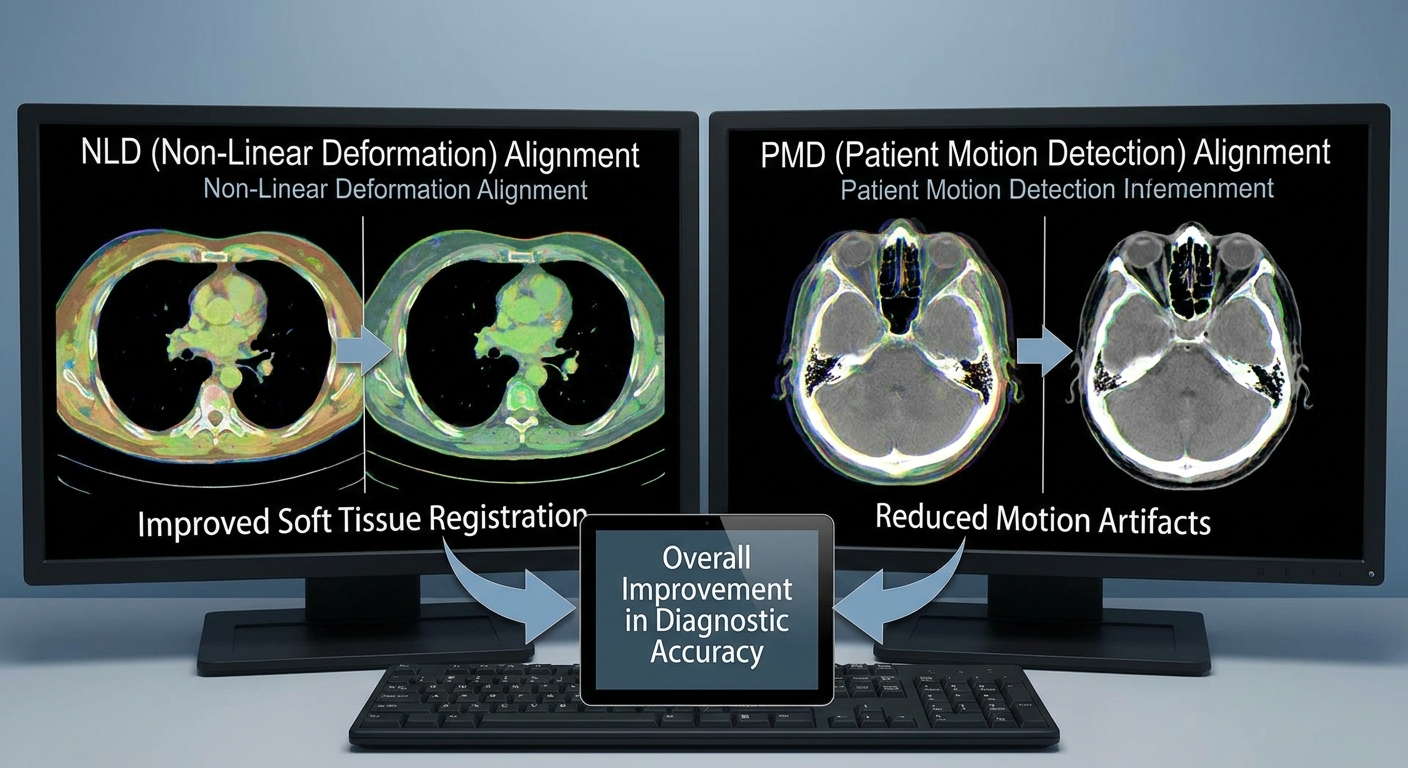
For patients who had CT scans, alignment improvements were measurable: 22% mean symmetry improvement at the nasolacrimal duct (NLD) level and 45% mean symmetry improvement at the point of maximal deviation (PMD), both statistically significant as reported by the authors.
How to interpret these checkpoints: the NLD level is a consistent anatomical landmark for comparing left-right airway space; the PMD is where the deviation is worst—often the spot most likely to affect airflow.
Citation: Dillard et al., 2026. doi:10.4193/RHINOL/25.018
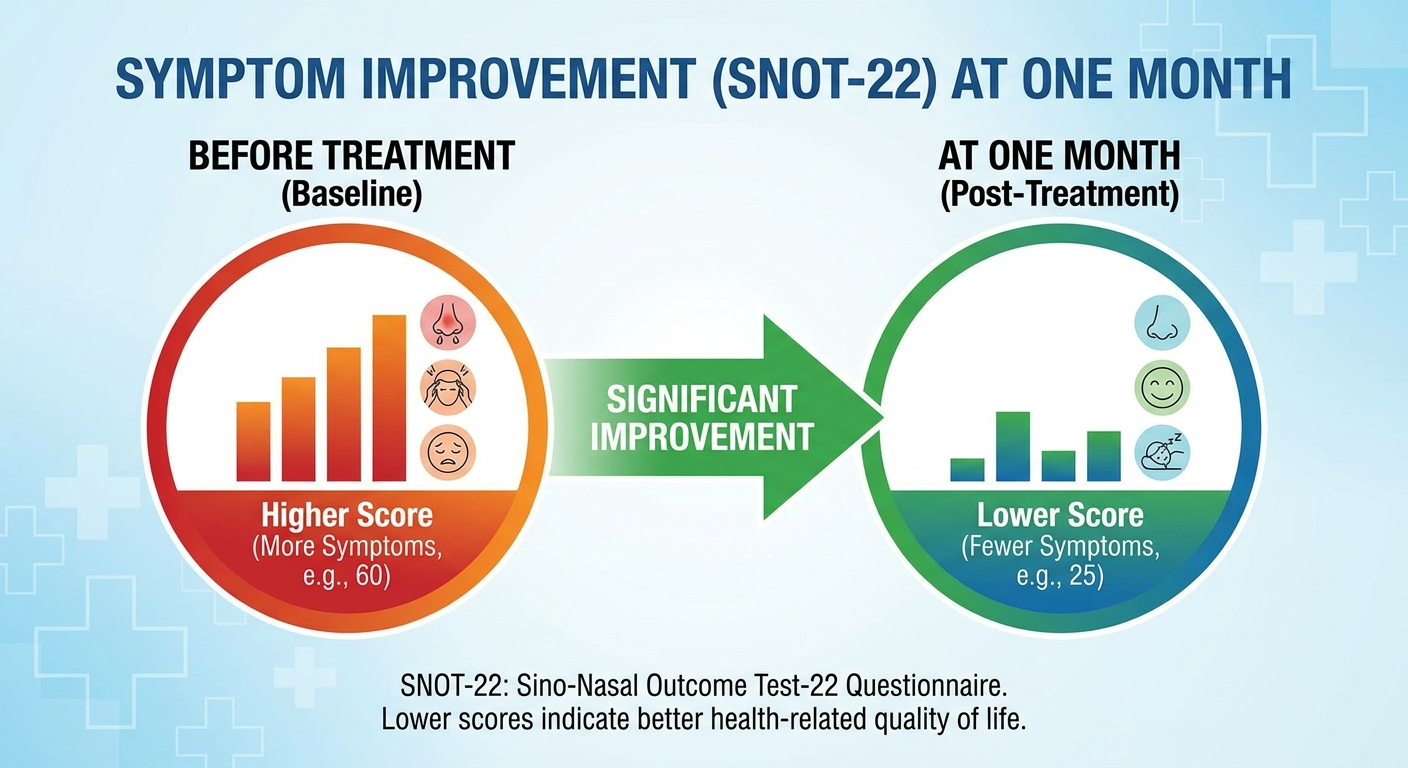
Symptom results: patients reported symptom improvement
SNOT-22 improved from 58.7 to 44.8 at one month (a 23.8% reduction).
If you’re unfamiliar with SNOT-22: https://www.clearpathnasal.com/blog/the-snot-22-score-measuring-your-sinus-health
Citation: Dillard et al., 2026. doi:10.4193/RHINOL/25.018
Safety signals in the cohort (what wasn’t seen)
In this retrospective review, no major complications were reported, including septal perforation, hematoma, mucosal injury, infection, synechiae, or conversion to traditional septoplasty.
This does not mean complications cannot occur in other patients or settings. Citation: Dillard et al., 2026. doi:10.4193/RHINOL/25.018
Who improved most?
Baseline severity mattered. Patients with severe deviation (>10 mm) showed the largest proportional alignment improvement, and 78% (18/23) achieved ≥30% alignment improvement (among those with CT data). Citation: Dillard et al., 2026. doi:10.4193/RHINOL/25.018
Takeaway: While “leapfrogging” isn’t a formal septum term, targeted, minimally invasive septal realignment can be tracked with imaging and symptom scores as reported by the authors.
When “Leapfrog” Language Might Be Used Informally (And What to Ask Your ENT)
Outside of published technique names, a clinician may use “leapfrogging” conversationally to describe correcting one area of deviation, then moving to the next; repositioning and re-supporting structures in sequence; or addressing multiple problem points rather than treating the septum as one uniform bend.
But again, the formal “leapfrog” term in the literature most strongly points to the Alar Leapfrog technique (cleft reconstruction), not a standard deviated septum procedure. Citation: PubMed PMID: 3905172.
Questions patients can bring to a consult
Which structure is being repositioned—septum, alar cartilage, or the nasal valve area? What approach is recommended and why (including whether a minimally invasive option such as balloon-assisted septoplasty with ClearPath is appropriate)? How will success be measured—exam/endoscopy, CT, or symptom scoring like SNOT-22? What risks are most relevant in my specific anatomy? What does recovery typically look like week by week?
A few clear questions can turn confusing jargon into a practical plan tailored to your anatomy and goals.
Key Takeaways (Patient Summary)
What “leapfrog” usually means
In published nasal surgery terminology, “leapfrog” most commonly refers to alar cartilage repositioning in cleft lip nasal reconstruction (the Alar Leapfrog technique). Citations: PubMed PMID: 3905172; ScienceDirect S0094129820316448.
What “segment-by-segment septum movement” should be understood as
Best understood as a patient-friendly way to describe targeted septal correction, not a single, formally named “leapfrog” septoplasty method.
Evidence-based reassurance
Modern septal realignment approaches can be tracked with objective alignment changes on CT, symptom improvement on validated tools such as SNOT-22, and clear reporting of safety outcomes in cohort data (limited to the studies cited).
Citation: Dillard et al., 2026. doi:10.4193/RHINOL/25.018
Net-net: focus less on the label “leapfrog” and more on what’s being corrected, how it’s measured, and whether it matches your anatomy.
Next Steps
If you suspect a deviated septum
If nasal blockage is affecting your breathing, sleep, or daily comfort, an ENT evaluation can help clarify whether symptoms are coming from a deviated septum, swelling/allergies, turbinate enlargement, nasal valve narrowing, or a combination.
From there, options may include medical therapy and, when appropriate, procedural correction—including balloon-assisted septoplasty with the ClearPath device as one minimally invasive septoplasty approach. ClearPath may be discussed as one alternative to traditional septoplasty, depending on anatomy, symptoms, and clinician judgment. Comparison: https://www.clearpathnasal.com/blog/clearpath-vs-traditional-septoplasty-recovery-safety-results
The right approach is the one that matches your anatomy, symptoms, and goals—with success measured objectively and subjectively.
Citations
Pigott RW. (1985). Alar “leapfrog” technique for cleft lip nasal reconstruction. PubMed PMID: 3905172. https://pubmed.ncbi.nlm.nih.gov/3905172/
Related summary/article page: ScienceDirect (S0094129820316448). https://www.sciencedirect.com/science/article/pii/S0094129820316448
Dillard J, Koudouovoh C, Lee V, et al. Outcomes of force-directed balloon-assisted endoscopic septoplasty: a retrospective analysis with a new technique and device. Rhinology Online. 2026;9:18–23. doi:10.4193/RHINOL/25.018
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.