

The Difference Between Rhinitis and Structural Blockage
Introduction: Why “Stuffy Nose” Isn’t One-Size-Fits-All
If you’re dealing with a “stuffy nose,” the cause (and the appropriate management) usually falls into one of two buckets:
- Inflammation inside the nose (rhinitis)
- Anatomy that physically narrows airflow (structural blockage)
Understanding the difference between rhinitis and structural blockage matters because each responds to different treatments—and many people actually have both, which is why symptoms can feel confusing or inconsistent. In many cases, care starts with your symptom history and a trial of medical therapy before moving on to specialized testing or an ENT evaluation (AAAAI, 2025; Mayo Clinic, 2024; Stanford Medicine, n.d.).
A simple way to think about it: rhinitis is like a swollen, irritated “filter lining” inside the nose, while structural blockage is more like a narrow doorway—so even if you calm inflammation, the doorway itself may still be tight.
For a related guide, see: deviated septum vs allergies (https://www.clearpathnasal.com/blog/deviated-septum-vs-allergies-how-to-tell-the-difference).
Bottom line: stuffiness can come from swelling, structure, or both—so matching symptoms to the cause is key.
What Is Rhinitis? (Inflammation Problem)
Definition—What’s happening inside the nose
Rhinitis means inflammation of the nasal lining. When that lining gets irritated, it can swell and produce extra mucus. The result is congestion, dripping, and that “blocked” sensation—even if the underlying nasal anatomy is normal (AAAAI, 2025; Mayo Clinic, 2024).
You can picture the nasal lining like a thin, moist “skin” that’s meant to warm and filter air. When it’s inflamed, it can act like a sponge—holding fluid and narrowing the space you breathe through.
Two major types are:
- Allergic rhinitis (immune system response to allergens)
- Nonallergic rhinitis (inflammation triggered by irritants, weather changes, or other non-allergy factors)
Common rhinitis symptoms (often “classic allergy” clues)
Rhinitis tends to create a recognizable pattern, especially when allergies are involved:
- Sneezing
- Itching (nose and/or eyes)
- Runny nose (often clear drainage)
- Congestion that often affects both sides
- Symptoms that come and go with seasons, exposures, or irritants (AAAAI, 2025; Mayo Clinic, 2024)
A concrete example: you might feel “fine” most mornings, then develop sneezing and a watery runny nose after cleaning a dusty room—or you might notice a predictable flare every spring when pollen counts rise.
Typical triggers
- Allergic rhinitis: pollen, dust mites, pet dander, mold
- Nonallergic rhinitis: smoke, strong odors, weather changes, pollution/irritants (AAAAI, 2025; Mayo Clinic, 2024)
Some people also notice nonallergic symptoms in specific situations—like stepping from cold outdoor air into a warm building, or being around strong fragrances. The key is that symptoms can be trigger-linked and variable, rather than fixed day after day.
Think “irritated and drippy” when symptoms fluctuate with triggers, especially if sneezing and itch are part of the picture.

What Is Structural Blockage? (Mechanical Narrowing Problem)
Definition—when anatomy physically restricts airflow
A structural blockage means there is an anatomic obstruction that narrows the nasal passages and restricts airflow. Medications can reduce swelling of the nasal lining, but they don’t reposition cartilage or bone (Stanford Medicine, n.d.; Advanced ENT & Allergy, n.d.).
This is a major reason the difference between rhinitis and structural blockage is so important: one is mainly an inflammation issue, and the other is a mechanical narrowing issue.
A helpful analogy: if rhinitis is a puffy inner lining, structural blockage is the frame being off—like trying to breathe through a straw that’s partly bent.
Common causes of structural nasal obstruction
Common contributors to nasal obstruction include:
- Deviated septum (the wall between nostrils is off-center)
- Inferior turbinate hypertrophy (enlarged turbinates reduce airflow space)
- Nasal polyps (soft tissue growths that can block airflow)
- Adenoid hypertrophy (more common in children) (Stanford Medicine, n.d.; Advanced ENT & Allergy, n.d.)
For a deeper dive on septal deviation, see: deviated septum explained (https://www.clearpathnasal.com/blog/deviated-septum-explained-symptoms-causes-and-modern-treatment-options).
Structural blockage symptoms (pattern clues)
Structural causes often feel different from rhinitis:
- Persistent airflow limitation (more “fixed” or constant)
- Often worse on one side (or noticeably changes with sleeping position)
- May not fully respond to typical allergy medications
- Can contribute to mouth breathing, snoring, and sleep disruption—especially when congestion becomes chronic (Stanford Medicine, n.d.)
For example, someone might say, “My left nostril has felt blocked for years,” or “I can breathe better if I sleep on a certain side.” That “steady, mechanical” quality is a clue.
Think “physically crowded” when blockage feels constant, one-sided, or positional—even on otherwise good days.

Rhinitis vs Structural Blockage: Key Differences (Quick Comparison)
What you feel (symptom profile)
- Rhinitis: congestion plus sneezing/itching/runny nose
- Structural blockage: more of a “can’t get air through” sensation that’s often steady
One patient-friendly way to separate them is to ask: Is this mostly a nose that’s irritated and drippy, or a nose that feels physically crowded even on good days?
What causes it
- Rhinitis: immune response (allergic rhinitis) or irritant-driven inflammation (nonallergic rhinitis)
- Structural: a deviated septum, turbinate hypertrophy, nasal polyps, or other anatomy physically narrowing the airway
What usually helps
- Rhinitis: trigger management plus medications (and sometimes immunotherapy)
- Structural: medical therapy may reduce swelling, but persistent obstruction may lead clinicians to discuss procedures such as septoplasty or turbinate reduction (AAAAI, 2025; Mayo Clinic, 2024; Stanford Medicine, n.d.)
In practice, symptoms and treatments tend to cluster into inflammation vs. structure—though many people have some of each.

The Overlap: Why You Can Have Both (and Why It Matters)
Allergies can make structural problems feel worse
Even if the main issue is structural, allergies can intensify the feeling of blockage. Allergic inflammation can swell the turbinates, reducing space even further—so a mild septal deviation may feel much more dramatic during allergy season (Stanford Medicine, n.d.; AAAAI, 2025).
This is why someone can feel “totally stuffed” in April, somewhat better in July, but still never feel fully clear year-round.
Why many clinicians treat inflammation first
Because swelling can “mask” what’s really going on structurally, many care plans start with a good trial of rhinitis therapy. If blockage persists after consistent treatment, that “leftover” obstruction can point toward a structural cause (Stanford Medicine, n.d.).
A common clinical mindset is: calm the lining first—then see what obstruction remains.

How Doctors Tell the Difference (Patient-Friendly Diagnostic Path)
Step 1—History and symptom pattern
Your symptom story often gives the first big clues:
- Seasonal vs year-round timing
- Specific triggers (pets, dust, pollen, smoke, strong odors)
- Whether symptoms improve with medications
- One-sided vs two-sided congestion (Stanford Medicine, n.d.; AAAAI, 2025)
If you can, bring specifics: which meds you tried, how long you used them, and whether you used nasal sprays daily (technique and consistency matter).
Step 2—Physical exam
A clinician may look for visible swelling, signs of turbinate hypertrophy, possible polyps, or clues suggesting a deviated septum (Stanford Medicine, n.d.). This step can also help spot “mixed” situations—for example, swollen turbinates on top of a septal deviation.
Step 3—Targeted testing when needed
When symptoms persist or the cause isn’t clear, testing may include:
- Allergy testing (skin or blood) to confirm allergic rhinitis triggers (AAAAI, 2025)
- Nasal endoscopy (a small camera to directly inspect the nasal cavity for septal deviation, turbinate enlargement, or nasal polyps) (Stanford Medicine, n.d.)
- CT scan of sinuses when structural disease is suspected or symptoms don’t improve as expected (Stanford Medicine, n.d.)
When people seek ENT evaluation sooner (red flags)
People often seek earlier ENT evaluation if they notice:
- Persistent one-sided blockage
- Symptoms that don’t improve with appropriate medical therapy
- Concern for polyps or significant anatomic narrowing (Stanford Medicine, n.d.)
Your story, exam, and focused tests together help separate swelling-driven symptoms from anatomy-driven airflow limits.
Treatment Options—What Works for Each Condition
Rhinitis treatments (medical-first approach)
For people whose symptoms are consistent with rhinitis, clinicians often recommend a consistent routine:
- Trigger avoidance and environmental controls
- Intranasal corticosteroids
- Oral, non-sedating antihistamines
- Ipratropium when runny nose is the main complaint
- Immunotherapy (allergy shots or tablets) when allergic triggers are confirmed (AAAAI, 2025; Mayo Clinic, 2024)
In everyday life, improvement often comes from doing the basics consistently rather than switching products frequently. For many people, a daily nasal steroid spray (used correctly) is a foundation therapy, especially for allergic rhinitis (AAAAI, 2025; Mayo Clinic, 2024).
Structural blockage treatments (when anatomy is the main issue)
If structural narrowing remains after treating inflammation, options clinicians may discuss include:
- Septoplasty (often for a deviated septum)
- Turbinate reduction / turbinoplasty (for turbinate hypertrophy)
- Polypectomy (for nasal polyps) (Stanford Medicine, n.d.; Advanced ENT & Allergy, n.d.)
If you’re exploring conservative strategies first, see: fix a deviated septum without surgery (https://www.clearpathnasal.com/blog/can-you-fix-a-deviated-septum-without-surgery).
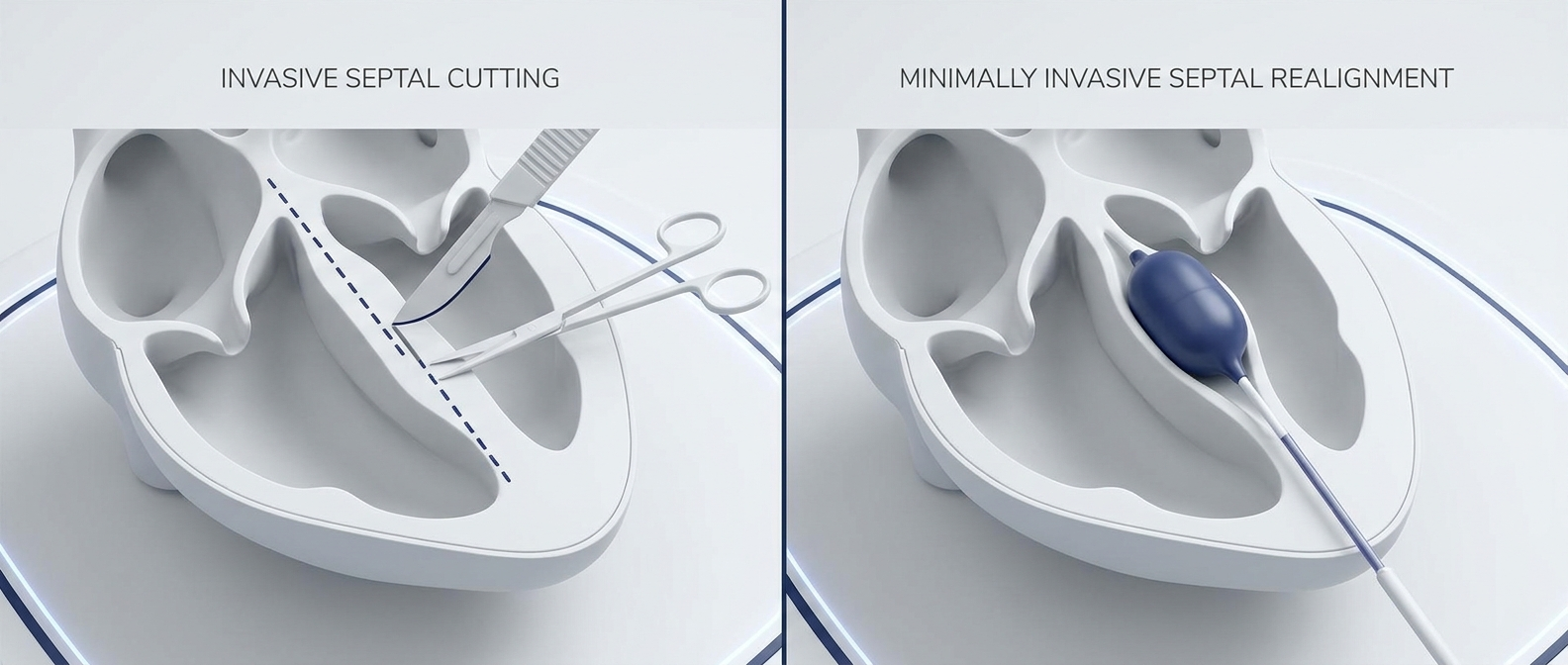
When surgery is appropriate, some surgeons may use minimally invasive, device-assisted septoplasty techniques depending on training, regulatory status, and patient anatomy. Availability varies by region and practice, and such techniques are not the standard in every setting. For an overview of one minimally invasive concept, see: balloon septoplasty (https://www.clearpathnasal.com/blog/what-is-balloon-septoplasty-a-minimally-invasive-option-for-deviated-septum).
Treat swelling first when appropriate; if fixed narrowing persists, clinicians may discuss procedures tailored to your anatomy and goals.
Evidence Snapshot: What Outcomes Can Look Like When Structural Blockage Is Addressed
When structural blockage is the main driver of symptoms, correcting the anatomy can improve airflow and quality-of-life measures. In a published review of 107 consecutive cases using a device-assisted, minimally invasive septoplasty technique sometimes associated with ClearPath, the authors reported:
- In a subgroup with CT scans, septal symmetry improved at key landmarks (22% and 45% improvements at specified points).
- No major complications were reported in that cohort (no perforation, hematoma, infection, or conversion to traditional septoplasty).
- Patient-reported symptoms improved at one month: SNOT-22 scores decreased from 58.7 to 44.8 (a 23.8% reduction).
- Some of the largest reported improvements included congestion, facial pressure/headache, and sleep quality (Dillard et al., 2026).
These findings describe outcomes in that specific cohort and technique, and should not be assumed to represent all septoplasty approaches or all patients.
Outcomes matter most when the diagnosis fits—i.e., when persistent blockage truly has a structural component that medical therapy alone can’t fully address.
Self-Check: Which One Sounds More Like You? (Not a Diagnosis)
Signs it may be rhinitis
- Itchy/sneezy/runny nose
- Symptoms tied to seasons or triggers
- Improves with antihistamines or nasal steroid sprays (AAAAI, 2025)
Signs it may be structural blockage
- Long-term obstruction, often worse on one side
- Little improvement despite consistent medical therapy
- Symptoms that feel positional (e.g., worse when lying on one side) (Stanford Medicine, n.d.)
If you’re unsure
Uncertainty is common—because overlap is common. Sorting out the difference between rhinitis and structural blockage often takes both a medical trial and an anatomy check.
If symptoms are mixed or confusing, it’s reasonable to explore both inflammation control and an anatomic evaluation.
When to Get Help (Practical Next Steps)
What people often try first (general guidance)
For those with symptoms suggestive of rhinitis, clinicians often emphasize:
- Consistent, correct use of nasal sprays (technique and daily use matter)
- Trigger reduction at home and work
- Following up if symptoms don’t improve after an appropriate trial (Mayo Clinic, 2024; AAAAI, 2025)
When to escalate care
It may be helpful to seek a clinical evaluation when:
- Obstruction persists after appropriate medical management
- Blockage is persistently one-sided
- You suspect polyps or significant structural narrowing
An ENT evaluation, nasal endoscopy, and sometimes a CT scan of the sinuses can help clarify whether anatomy is the main issue—and whether procedures like septoplasty or turbinate reduction are worth discussing (Stanford Medicine, n.d.; Mayo Clinic, 2024).
If symptoms persist despite appropriate treatment, a focused evaluation can help determine whether the problem is inflammation, structure, or both.

FAQ (SEO-Friendly)
Can allergies cause a deviated septum?
No. A deviated septum is structural (anatomy). However, allergies can swell nasal tissues and make a pre-existing deviation feel more obstructive (Stanford Medicine, n.d.; AAAAI, 2025).
Why do I feel blocked if my allergy meds help only a little?
This can happen with mixed disease: inflammation improves, but a structural narrowing (like turbinate hypertrophy or septal deviation) still limits airflow (Stanford Medicine, n.d.).
Do nasal sprays fix structural blockage?
Nasal sprays can reduce swelling and mucus, which may temporarily improve airflow. They may also reduce inflammation and sometimes shrink polyps, but they do not permanently correct a deviated septum (Stanford Medicine, n.d.; AAAAI, 2025).
References
- American Academy of Allergy, Asthma & Immunology (AAAAI). Hay Fever / Rhinitis. 2025. https://www.aaaai.org/conditions-treatments/allergies/hay-fever-rhinitis
- Mayo Clinic. Hay fever (Allergic rhinitis). 2024. https://www.mayoclinic.org/diseases-conditions/hay-fever/symptoms-causes/syc-20373039
- Stanford Medicine Otolaryngology—Head & Neck Surgery. Nasal Obstruction (Patient Guide). n.d. https://med.stanford.edu/ohns/OHNS-healthcare/sinuscenter/resources/patient_guides/nasal-obstruction.html
- Advanced ENT & Allergy. Nasal Septal Deviation and Turbinate Hypertrophy. n.d. https://www.entallergy1.com/contents/our-services/nasal-septal-deviation-and-or-turbinate-hypertrophy
- Dillard J, Koudouovoh C, Lee V, et al. Rhinology Online. 2026;9:18–23. doi:10.4193/RHINOL/25.018
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.