

The 7 Types of Septal Deformities: The Mladina Classification
If you’ve been told you have a “deviated septum,” it’s natural to ask: What kind of deviation do I have—and does the shape matter?
Your nasal septum is the wall of cartilage and bone that divides your nose into left and right sides. When that wall is bent, ridged, or develops a spur, it can narrow airflow and contribute to symptoms like congestion, mouth breathing, snoring, or a “blocked on one side” feeling. For a helpful overview of symptoms and causes, see deviated septum symptoms and causes: https://www.clearpathnasal.com/blog/deviated-septum-explained-symptoms-causes-and-modern-treatment-options
A helpful analogy: if your nose is a two-lane hallway, the septum is the center divider. A small “dent” in the wrong place can feel worse than a bigger bend elsewhere—especially if it happens near the front where airflow is already tight.
What many people don’t realize is that a deviated septum isn’t just one shape. There are multiple septal deformities—and different patterns can create different “pinch points” for airflow and influence septoplasty planning. One widely used way ENTs describe these patterns is the Mladina classification (Mladina, 2015).
What Is the Mladina Classification (and Why Does It Matter)?
A simple way to group septal deformities into 7 patterns
The Mladina classification divides common deviated septum types into seven patterns:
- Types 1–4 are “vertical” deformities
- Types 5–6 are “horizontal” deformities
- Type 7 is a combination of multiple patterns
This “vertical vs horizontal” framework is popular in clinical literature because it’s practical and reproducible (Mladina, 2015; Teixeira et al., 2016). In other words, it gives clinicians a shared vocabulary for describing what they’re seeing, not just a vague label of “deviation.”
How ENTs use it clinically
In real-world visits and surgical planning, identifying the type can help an ENT anticipate:
- Where airflow is blocked (front/nasal valve area vs deeper in the nose)
- What else may be contributing (like turbinate enlargement or concha bullosa in some patterns)
- How complex correction may be, especially for high/deeper deviations or mixed Type 7 cases (Mladina, 2015)
You might even hear a clinician summarize it like this: “The important part isn’t just that it’s deviated—it’s where the narrowest point is.” That “narrowest point” often explains why two people with the same CT report can feel very different day to day.
— In short: location and shape often matter more than the word “deviated.” —

How Common Is Septal Deviation?
Why prevalence numbers vary so much
Studies report a wide range of prevalence, in part because the definition of “deviation” varies and because improved exams/imaging detect smaller deformities. Some populations show rates as high as ~86% (Alghamdi, 2022).
Just as important: common doesn’t always mean symptomatic. Many people have a deviation that never becomes a meaningful breathing problem. Symptoms tend to show up when the deviation combines with swelling (allergies, colds), enlarged turbinates, nasal valve narrowing, or other anatomy that reduces the “spare space” inside the nose.
— Bottom line: deviated septum is common, but only treated when symptoms and function warrant it. —
The 7 Mladina Types (Plain-English Guide)
At-a-glance summary (Type → what it looks like → where it tends to block)
- Type 1: Mild vertical ridge near the front → Subtle, early narrowing at the front
- Type 2: Vertical ridge reaching the nasal valve → Valve “bottleneck” involvement
- Type 3: Deeper/high vertical deviation → Narrowing deeper in the nasal cavity
- Type 4: S-shaped septum → Multiple levels; can feel alternating
- Type 5: Almost-horizontal ridge or nasal septum spur → Localized contact/irritation
- Type 6: Large unilateral bony (vomeral) spur → One-sided, rigid obstruction
- Type 7: Combination (“mixed”) → Variable; depends on components
Type 1 — Mild vertical ridge near the front, not reaching the valve
What it is: A unilateral vertical ridge in the nasal valve region that does not reach or touch the nasal valve.
What you may feel: Intermittent blockage, often worse with colds, allergies, or seasonal swelling—sometimes subtle. People may describe it as “fine most days, then randomly annoying.”
What an ENT may check: Early narrowing at the front of the nose and whether swelling (not structure) is doing most of the work (Mladina, 2015).
Type 2 — Vertical ridge that reaches/touches the nasal valve
What it is: A vertical ridge that reaches the nasal valve, one of the highest-resistance airflow zones.
What you may feel: Stronger one-sided obstruction, trouble breathing during exercise, or worsening at night. Some patients notice they instinctively pull a cheek to the side to open the airway.
Why it matters: Involvement of the nasal valve can amplify symptoms even if the septum doesn’t look dramatically “crooked” (Mladina, 2015). Think of the valve like a doorway: a small obstruction at the doorway can restrict flow more than a larger issue deeper inside.

Type 3 — Deeper vertical ridge / “high” deviation
What it is: A vertical ridge located deeper in the nasal cavity—often described as a high deviation.
What you may feel: Persistent blockage that nose strips don’t help much, because the narrowing is not primarily at the nostril opening. Some people say, “It feels blocked behind my nostril.”
Common associated findings: Concha bullosa and turbinate hypertrophy are reported more commonly with Types 3 and 4 (Mladina, 2015; Teixeira et al., 2016).
Planning note: Deeper/high deviations can be more technically challenging, which can affect surgical approach (Mladina, 2015).
Type 4 — “S-shaped” deviation (antero-posterior S)
What it is: An S-shaped septum, where different parts of the septum bend in different directions.
What you may feel: Alternating blockage (one side then the other) or a sense that “both sides feel tight,” especially when lying down.
Common associated findings: As with Type 3, concha bullosa and turbinate hypertrophy may be more frequent (Mladina, 2015). In practice, an ENT is often looking for multiple contributing “pinch points,” not just one.

Type 5 — Almost-horizontal septal spur/crest
What it is: A more horizontal ridge or nasal septum spur—often a pointier projection than a smooth curve.
What you may feel: Localized obstruction, irritation, crusting, or “contact-point” discomfort in some people. Patients sometimes describe a “scratchy” or “tender” spot on one side.
Biology note: Type 5 has been reported to show evidence of heritability in some research—meaning a genetic contribution may play a role in certain families (Mladina, 1987; Mladina, 2015).

Type 6 — Massive unilateral bony (vomeral) spur
What it is: A larger, more rigid bony spur, often described as vomer-related.
What you may feel: Significant one-sided blockage and sometimes turbulent airflow that feels dry or irritating. Because it’s rigid, it may feel less “variable” day to day than swelling-driven congestion.
Why it matters: Rigid bony components may influence what correction methods are appropriate (Mladina, 2015).
Type 7 — Combination (“mixed” deformity)
What it is: A combination of multiple deviation patterns—sometimes described as “crumpled” or mixed.
What you may feel: More variable symptoms, depending on which components dominate (valve narrowing, high deviation, spurs, etc.).
How common is it? Type 7 is reported as one of the most common types in some series (Mladina, 2015; Alghamdi, 2022). Clinically, it’s also one of the reasons two “deviated septum” cases can be very different in complexity.
— Different types create different pinch points; your symptoms usually follow the narrowest spot. —

What Other Problems Can “Travel” with a Deviated Septum?
Turbinate hypertrophy (enlarged turbinates)
Turbinates help warm and humidify air. When airflow is uneven, turbinates can enlarge as the nose tries to regulate airflow—sometimes worsening obstruction. This has been reported more commonly with Types 3 and 4 (Mladina, 2015).
Concha bullosa (air-filled middle turbinate)
A concha bullosa is an air-filled enlargement of the middle turbinate. If it’s large, it can take up space and worsen blockage—again reported more often with Types 3 and 4 (Mladina, 2015).
Nasal valve narrowing
The nasal valve (front of the nose) is a key bottleneck for airflow, and even small changes there can feel significant—especially relevant to Types 1–2. This is one reason an exam that focuses only on the “back” of the nose can miss what’s driving symptoms.
— Other structures (turbinates, concha bullosa, the nasal valve) can magnify the impact of a deviation. —
How ENTs Diagnose Septal Deformity Type
Office exam plus nasal endoscopy
Diagnosis usually starts with a focused history and exam. Many ENTs use nasal endoscopy—a small camera—to see deeper structures and locate the real “pinch point.” During a visit, you may notice the clinician comparing sides, looking at the nasal valve region, and checking whether turbinates are enlarged. They’re essentially mapping where the airflow is getting crowded.
When CT imaging is used (and when it isn’t)
CT scans aren’t necessary for every deviated septum. They’re often used when sinus disease is suspected or when surgery is being planned, because CT can show deeper anatomy and related findings.
Why “type” matters more than a single word like “deviated”
A single label (“deviated”) can miss the most important details: location, shape, and whether spurs or high deviations are present. Those details help explain why some people improve with medical therapy while others don’t (Teixeira et al., 2016).
— Pinpointing the type helps match treatment to the true site of airflow resistance. —
Treatment Options (From Symptom Control to Structural Correction)
When medical therapy can help
If swelling is a major contributor, symptom control may include saline rinses, allergy management, and anti-inflammatory nasal sprays. These won’t “straighten” cartilage or bone, but they can reduce tissue swelling around a deviation—especially when symptoms spike seasonally or fluctuate week to week.
When septoplasty may be considered
Septoplasty may be discussed when symptoms persist—such as ongoing obstruction, sleep disruption, or recurrent congestion despite appropriate medical therapy. A practical benchmark many patients relate to is: “If I’m constantly planning my day around breathing through one side of my nose, it’s time to talk options.” The decision is individualized and should be based on function and quality of life—not the exam finding alone. For more on how anatomy influences results, see septoplasty outcomes by deviation type: https://www.clearpathnasal.com/blog/septoplasty-outcomes-by-deviation-type-mladina-classification
Surgical planning: different deviation types may call for different approaches
From a patient perspective, the key idea is simple: different deformities live in different places.
- Some deviations are mainly at the front (nasal valve area)
- Others are deeper/higher (Types 3–4)
- Some involve spurs (Types 5–6)
- Some are mixed (Type 7)
Your surgeon also considers turbinates, nasal valve support, prior trauma, and your goals (Mladina, 2015).
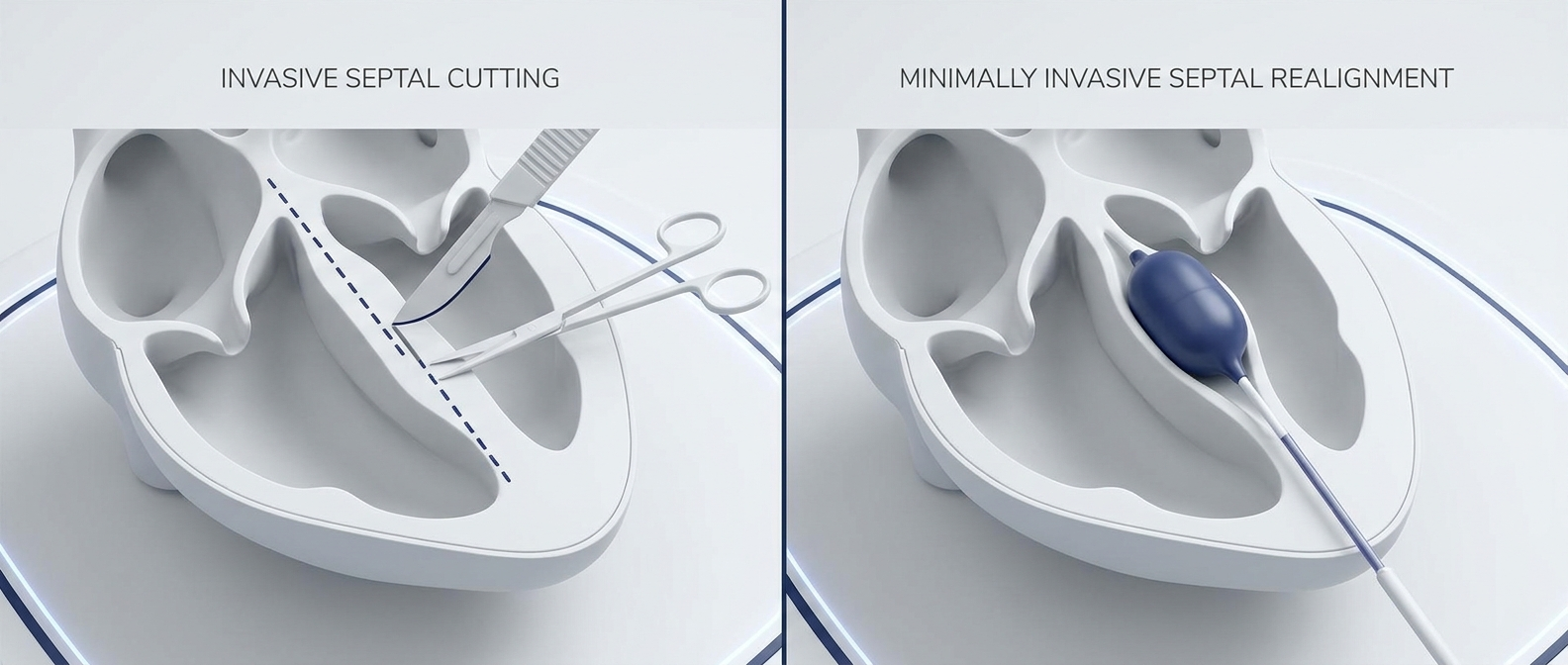
Where minimally invasive, endoscopic techniques may fit (including balloon-assisted approaches)
In some patients, minimally invasive, endoscopic approaches may help correct specific patterns while aiming to reduce tissue disruption. One example is balloon-assisted endoscopic septoplasty using the ClearPath device, which has shown promising early outcomes in retrospective studies, although further research is ongoing. In one retrospective series of 107 cases, force-directed, balloon-assisted endoscopic septoplasty using a ClearPath system reported no major complications observed and symptom improvement (SNOT-22) at follow-up; in a subset with CT comparisons, septal alignment improved at measured levels (Dillard et al., 2026). Here, “force-directed” refers to controlled, instrument-guided pressure applied during balloon expansion to mobilize targeted cartilage or bony deviations. Candidacy depends on your anatomy, severity, and your surgeon’s assessment. For background reading, see What is balloon septoplasty?: https://www.clearpathnasal.com/blog/what-is-balloon-septoplasty-a-minimally-invasive-option-for-deviated-septum
— The best plan treats the bottleneck you actually have—sometimes with medication alone, sometimes with structural correction. —
Questions to Ask Your ENT (Bring This to Your Visit)
- Which Mladina type do I have—and where is the main blockage?
- Do I also have turbinate hypertrophy or concha bullosa?
- Is my nasal valve involved?
- Would my deviation be better treated with a minimally invasive approach or a more traditional septoplasty technique?
- What recovery and symptom improvement should I realistically expect?
FAQ
What is the Mladina classification used for?
The Mladina classification is used to group septal deformities into seven common patterns, helping ENTs communicate what the deviation looks like and plan treatment based on location and shape (Mladina, 2015).
Which septal deviation types are linked to concha bullosa or turbinate hypertrophy?
Research reports these findings more commonly in Types 3 and 4 (Mladina, 2015).
Can a deviated septum be genetic?
Sometimes. Evidence of heritability has been reported for Type 5 in some research, suggesting genetics can contribute in certain families—but many deviations are also influenced by growth patterns and/or trauma (Mladina, 1987; Alghamdi, 2022). For more context, see Is a deviated septum genetic or acquired?: https://www.clearpathnasal.com/blog/is-a-deviated-septum-genetic-or-acquired
Is septal deviation always a problem that needs surgery?
No. Septal deviation is common and often asymptomatic. Treatment is based on symptoms and functional impact, not the CT or exam finding alone.
Conclusion + Next Step
A deviated septum isn’t one-size-fits-all. The Mladina classification breaks septal deformities into seven patterns, helping explain where airflow is blocked and why symptoms can differ from person to person. Understanding your deviation type—whether it’s valve-related, a high deviation, an S-shaped septum, or a nasal septum spur—can make conversations about next steps clearer and more productive.
If you’re still struggling with nasal blockage, ask your local ENT to explain which Mladina type you have and to review both traditional septoplasty options and minimally invasive alternatives—such as balloon-assisted endoscopic septoplasty—based on your anatomy and goals.
— Clarity on your type empowers a treatment plan tailored to how you actually breathe. —
Medical disclaimer
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
References
1. Mladina R. The role of maxillar morphology in the development of pathological septal deformities. Rhinology. 1987. https://www.rhinologyjournal.com/Rhinology_issues/639.pdf
2. Mladina R. Clinical Implications of Nasal Septal Deformities. Int J Clin Pract. 2015. https://pmc.ncbi.nlm.nih.gov/articles/PMC4737055/
3. Teixeira J, et al. Nasal Septal Deviations: A Systematic Review of Classification Systems. 2016. https://pmc.ncbi.nlm.nih.gov/articles/PMC4432693/
4. Alghamdi FS. Nasal Septal Deviation: A Comprehensive Narrative Review. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC9736816/
5. Dillard JD, Koudouovoh C, Lee V, et al. Outcomes of force-directed balloon-assisted endoscopic septoplasty… Rhinology Online. 2026;9:18–23. doi:10.4193/RHINOL/25.018
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.