

Identifying “Cottle’s Areas” in the Nose (1–5)
Feeling “stuffy” can mean very different things inside the nose. One person’s blockage may be right at the nostril opening, while someone else’s may come from deeper, narrow internal structures—yet both describe the same symptom: “I can’t breathe through my nose.”
One educational framework some ear, nose, and throat (ENT) clinicians use to describe where airflow may be restricted is Cottle’s areas—five zones that help localize a likely obstruction site and guide discussion of treatment options. Think of it like narrowing down which segment of a hallway is causing a bottleneck: the front door, the tight corner, or the back corridor.
Why “where” your nose is blocked matters
Nasal obstruction isn’t one problem
“Nasal obstruction” is a symptom, not a single diagnosis. Congestion can come from different internal zones (front vs. middle vs. back), and many issues can produce similar day-to-day complaints, such as:
- Stuffiness (on one side or both)
- Mouth breathing (especially at night)
- Poor sleep or snoring
- Sinus pressure or facial discomfort
- A “blocked in the back” sensation with postnasal drip
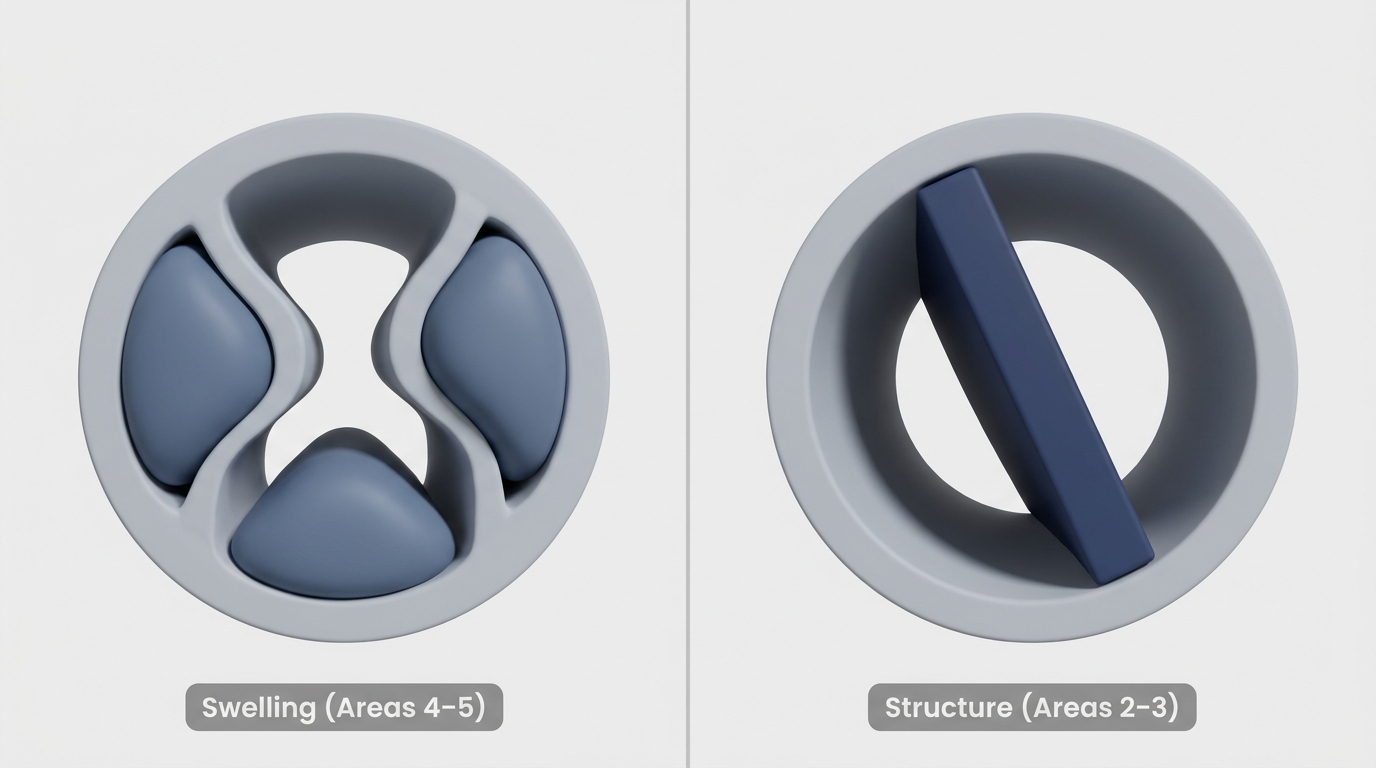
Sometimes the cause is mainly soft tissue swelling (for example, allergies). Other times it’s structural narrowing (for example, a deviated septum). An easy analogy: swelling is like the walls of a hallway “puffing inward,” while a septal deviation is like the hallway being built slightly crooked. For a simple primer on structure, see deviated septum anatomy and how it affects airflow: https://www.clearpathnasal.com/blog/deviated-septum-causes-understanding-your-nasal-anatomy
How clinicians use anatomic “maps”
Because symptoms can overlap, clinicians rely on anatomic frameworks to describe nasal obstruction location more clearly. Cottle’s areas are a commonly taught educational framework in ENT training and are often shown in teaching diagrams and figures. They’re especially helpful when discussing functional procedures like septoplasty and nasal valve repair.
A clinician may essentially be answering, “Is this an entry problem, a valve problem, or a deeper cavity problem?” That location-based thinking can help keep treatment options targeted rather than one-size-fits-all.
References: The ENT Resident teaching summary and commonly reproduced figures show the five-zone concept. (See sources listed at the end.)
Bottom line: Pinpointing “where” the blockage occurs can clarify why the same symptom may need very different solutions.

What are Cottle’s Areas? (The 5-zone classification)
In patient-friendly terms: Cottle’s classification divides the inside of the nose into five areas to help consider where airflow is most restricted.
Quick overview of Areas 1–5 (one sentence each)
- Area 1: The nostril opening (the entry point).
- Area 2: The nasal valve area (the narrow functional “pinch point”).
- Area 3: The upper internal nasal cavity under the bony-cartilaginous “vault.”
- Area 4: The anterior cavity (front internal cavity—includes the front portions of the turbinates and nearby drainage pathways).
- Area 5: The posterior cavity (back of the nose—includes the posterior portions of the turbinates).
Visual suggestion (optional): Consider adding a simple labeled diagram based on a published figure of Cottle’s classification (see Open-i and Huizing figure links in References).
Think of Areas 1–5 as a teaching map—useful for conversation, not a standalone diagnosis.
How to identify each Cottle Area (what it is + what blockage may feel like)
Important note: “What it feels like” can be a clue, not a diagnosis. Two people can have the same anatomic issue and describe it differently—and vice versa.
Area 1 (Nostril) — the “front door”
What it is: The rim and opening of the nostril itself.
Common issues:
- Soft-tissue collapse at the nostril rim (sometimes more noticeable on a deep inhale)
- Swelling of the skin/lining at the opening
- Scarring (for example, from trauma or prior procedures)
What it may feel like: Blockage seems right at the entrance, and some people notice improvement when they gently flare their nostrils.
Concrete example: A patient might say, “It feels like the opening is too small—like breathing through a partially pinched straw.” Descriptions like this can be consistent with Area 1 involvement (and sometimes Area 2).
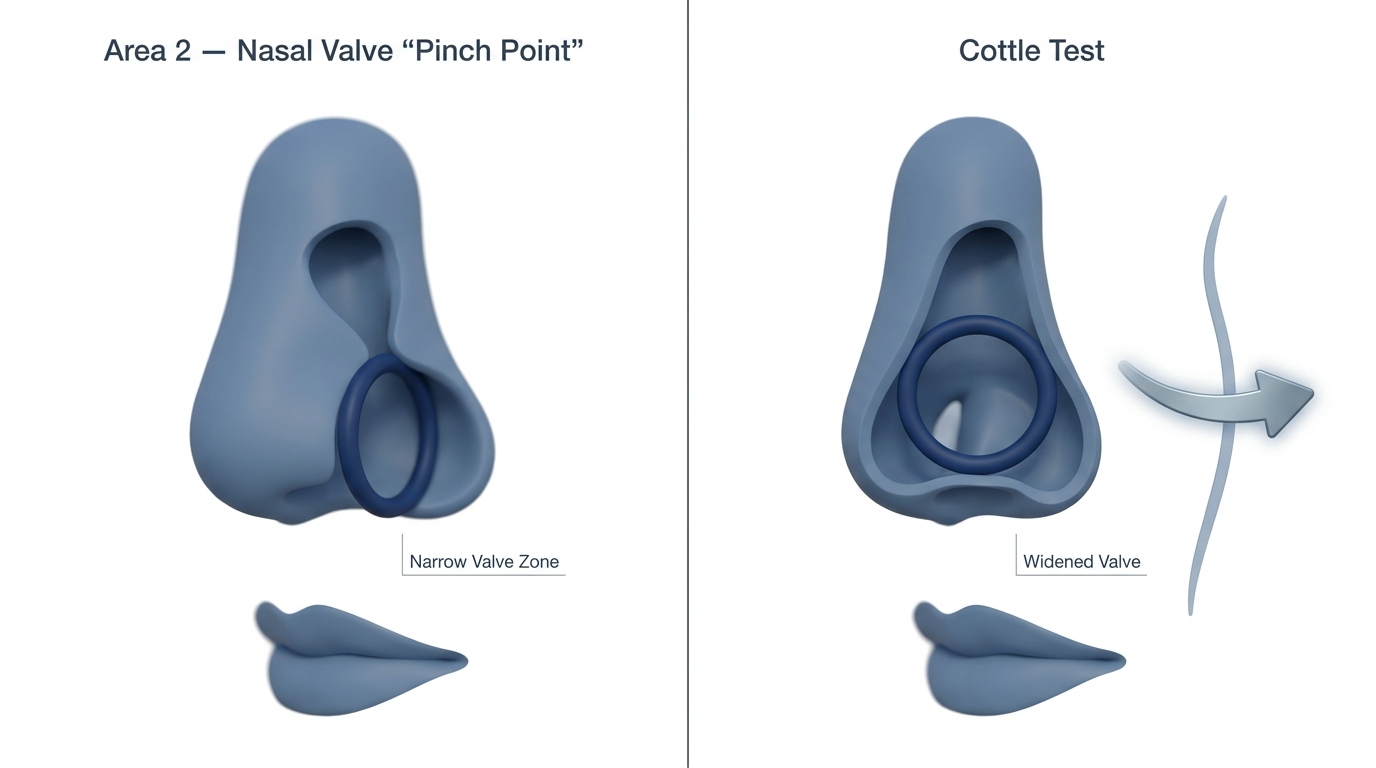
Area 2 (Nasal valve) — the most common “pinch point”
What it is: The nasal valve area, often described as the narrowest functional segment for airflow in the front-to-middle nose. Small changes here can have a big impact on perceived breathing.
Why it matters: Airflow resistance rises quickly when a narrow segment gets even narrower—so mild structural narrowing or dynamic collapse can feel dramatic. Many people notice this most when exercising, taking a deep breath, or lying down.
The Cottle test (simple in-office maneuver)
One classic screening maneuver tied to Area 2 is the Cottle test:
- How it’s done: A clinician gently pulls the cheek laterally (to the side) to slightly widen the nasal valve region and asks whether breathing improves.
- What a “positive” result can mean: A positive result may suggest nasal valve involvement, but it is not specific and must be interpreted with the rest of the exam.
- Important caveat: The Cottle test is a screening tool, not a complete diagnosis. A negative test does not rule out other internal narrowing.
Patient-style phrasing you might hear: “When I pull my cheek to the side, I can finally get air in.” That’s the basic logic behind the maneuver—temporarily widening a potential pinch point to see if airflow changes.
Reference: The association of the Cottle test with the nasal valve region is commonly taught in ENT resources. (See The ENT Resident link in References.)
Area 3 (Upper internal cavity) — under the “vault”
What it is: Think of this as an “upper corridor” under the nasal bones and upper cartilages (the internal vault). This is part of internal nasal anatomy that’s hard to judge without an exam.
Common issues:
- A high septal deviation (higher up than people expect)
- Swelling of the lining in the upper internal nose
What it may feel like: Congestion may feel deeper than the nostril and can be difficult to localize by sensation alone. People sometimes describe it as a vague “tightness” rather than classic runny-nose congestion.
Clinician reality check: This is one reason ENTs often say, “Your symptoms tell me it’s obstructed—but the exam tells me where.”
Area 4 (Anterior cavity) — turbinate heads & drainage pathways
What it is: The front internal cavity that includes the front portions (heads) of the turbinates and nearby drainage pathways (often described in relation to the infundibulum region).
Turbinates in plain language: Turbinates are normal structures that help warm, humidify, and filter air. They contain tissue that can swell and shrink, which is useful for normal nasal function—but frustrating when swelling becomes persistent.
Common issues:
- Allergic inflammation
- Irritant exposure
- Viral illness
- Chronic rhinitis
What it may feel like: Congestion can alternate sides, flare seasonally, or come with pressure around the cheeks/eyes—especially when inflammation is driving the swelling.
If you’re trying to sort out inflammation vs. structure, this comparison can help: deviated septum vs allergies: how to tell the difference: https://www.clearpathnasal.com/blog/deviated-septum-vs-allergies-how-to-tell-the-difference
Concrete example: A person might report, “I’m fine in the morning, but by afternoon one side shuts down—then later it switches.” Patterns like this may prompt clinicians to look closely at turbinate tissue behavior.
Area 5 (Posterior cavity) — the back of the nose
What it is: The back portion of the nasal cavity, including the posterior portions (“tails”) of the turbinates as airflow moves toward the throat.
Common issues:
- Posterior septal deviation
- Inflammation that’s worse deeper in the nose
- Ongoing rhinitis with postnasal drainage
What it may feel like: People often describe this as “blocked in the back,” with postnasal drip, throat clearing, or nighttime mouth breathing.
Practical clue: If someone says, “I can’t move air through the back of my nose even when I’m not runny,” clinicians may consider whether posterior anatomy (or deeper inflammation) is playing a bigger role than what’s visible at the nostrils.
Reference for Areas 1–5 definitions: The five-zone description is commonly reproduced in educational figures. (See Open-i figure in References.)
Symptoms can hint at location, but the exam is what localizes obstruction reliably.
How ENT clinicians confirm the “area” causing obstruction

The exam tools patients should know
Because symptoms can be misleading, clinicians typically use a combination of:
- Anterior rhinoscopy (nasal speculum exam): A front-of-nose view to assess septum position, swelling, and the front turbinates.
- Nasal endoscopy: A small camera exam that looks deeper—helpful for the posterior cavity (Area 5) and other regions that can’t be seen well from the front.
- Imaging (CT): Not required for everyone, but sometimes used when sinus anatomy, complex deviation, or deeper structural questions are involved.
Why symptoms alone can mislead
A “congested” feeling may come from:
- Swollen lining/turbinates (soft-tissue narrowing), or
- Structural narrowing (septum deviation, nasal valve area collapse), even when there isn’t much mucus.
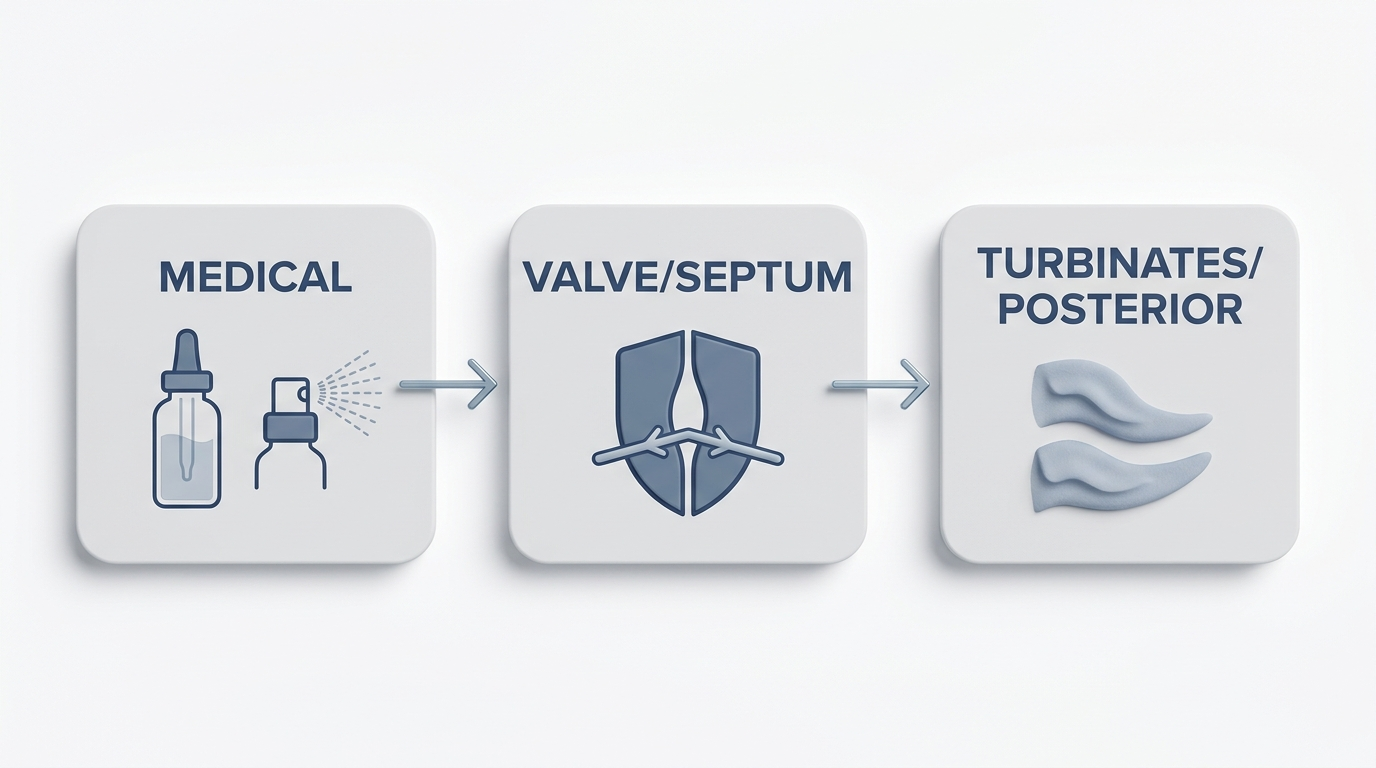
That’s why localizing the problem using anatomic concepts such as Cottle’s areas can be helpful—especially when deciding whether the next step is medical therapy, a procedure, or both.
An in-office exam plus endoscopy, when needed, is the most direct way to confirm the true blockage site.
How Cottle’s Areas guide treatment (from conservative care to procedures)
If the problem is mostly Areas 4–5 (inflammation-driven)
When swelling and inflammation are the main drivers—often in Areas 4 and 5—clinicians commonly start with conservative options, such as:
- Saline rinses
- Allergen avoidance and allergy management (when relevant)
- Topical medications (as appropriate for your situation)
When to reassess: If symptoms persist despite a reasonable trial, or if blockage is one-sided, worsening, or associated with frequent infections, an exam can help confirm whether a structural issue is also present.
To help compare inflammatory vs structural causes, see deviated septum vs allergies: how to tell the difference: https://www.clearpathnasal.com/blog/deviated-septum-vs-allergies-how-to-tell-the-difference
If the problem is structural (often Areas 2–3, sometimes 4)
Structural narrowing can limit airflow even without classic “congestion.” This can include:
- Septal deviation (which may affect more than one area)
- Narrowing or collapse in the nasal valve area
- Higher (upper) narrowing that’s not obvious without endoscopy
Depending on the findings, a clinician may discuss procedural options such as septoplasty and/or techniques focused on the nasal valve or turbinates, tailored to the anatomy and symptoms.
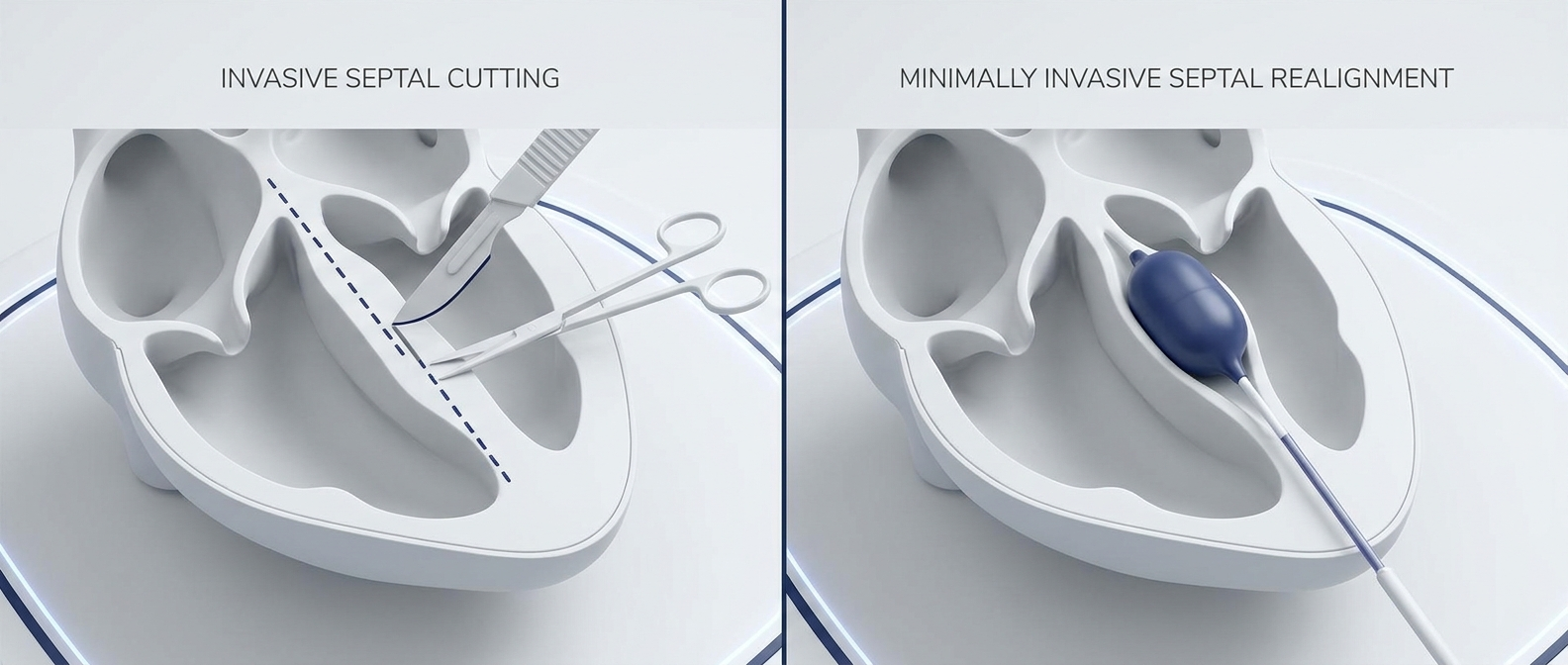
Where balloon septoplasty fits into the conversation (patient-friendly)
Some clinicians may consider balloon-based techniques in selected patients, depending on anatomy and the specific obstruction being treated. For general background, see:
- what is balloon septoplasty? https://www.clearpathnasal.com/blog/what-is-balloon-septoplasty-a-minimally-invasive-option-for-deviated-septum
- balloon septoplasty vs traditional septoplasty https://www.clearpathnasal.com/blog/clearpath-vs-traditional-septoplasty-recovery-safety-results
Positioning note (neutral): Depending on anatomy, a clinician may discuss a range of procedural options—such as traditional septoplasty, valve-focused repair, turbinate procedures, or, in selected cases, balloon-based approaches—to determine what is appropriate.
Clinical evidence callout (context and caution)
A retrospective review reported outcomes in 107 consecutive balloon-assisted septoplasty cases. In a small CT-imaging subgroup (n=23), septal alignment metrics improved at certain landmarks, and patient-reported SNOT-22 scores decreased at 1 month. No major complications were reported in that cohort; however, all procedures carry risks. Because the study was retrospective, non-randomized, and included a small imaging subgroup with short follow-up, results should be interpreted cautiously and may not generalize to all patients. Reference: Dillard et al., Rhinology Online (2026).
Treatment is most effective when it’s matched to the exact site and cause of narrowing identified on exam.
Is Cottle’s classification still used? (And why some experts simplify it)
Why it’s taught
Even today, Cottle’s areas give clinicians a shared language for describing likely blockage sites and discussing functional planning—especially around the nasal valve area.
The modern critique
Some rhinology reviews note that the five-area terminology can be confusing and propose simplified frameworks (for example, broader anterior/middle/posterior segments). Huizing’s review is often cited and includes a commonly reproduced figure. (See References.)
Cottle’s areas are a helpful teaching tool, but clinicians may also use simpler, anatomy-based descriptions in practice.
When to see an ENT (practical checklist)
Consider evaluation if you have:
- Obstruction most days for more than 8–12 weeks
- Mouth breathing or sleep disruption
- Frequent sinus infections or persistent facial pressure
- History of nasal trauma or suspected septal deviation
What to ask at your appointment:
- “Which area seems most narrowed on exam—nostril, nasal valve, septum, turbinates, or the posterior nose?”
- “Would nasal endoscopy help identify the obstruction site more clearly?”
- “Based on my anatomy, what medical and procedural options should we consider, and how do they compare?”
Prepare a few focused questions—location and cause will guide your next steps.
FAQs
What is the nasal valve (Cottle Area 2)?
The nasal valve is a naturally narrow part of the nasal airway where small changes in shape or support can significantly affect airflow. It’s often discussed as a key potential “pinch point.”
What is the Cottle test and what does a positive result mean?
The Cottle test gently pulls the cheek outward to temporarily widen the nasal valve region. If breathing improves, it may suggest nasal valve involvement. It is a nonspecific screening maneuver and should be interpreted alongside the full exam.
Can a deviated septum affect more than one Cottle area?
Yes. A septal deviation can narrow airflow at different depths and heights, potentially influencing multiple zones—one reason a full evaluation of internal nasal anatomy matters.
Are turbinates part of Cottle’s areas?
Yes. Turbinates are most relevant to Areas 4 and 5 (front “heads” and back “tails”). They’re normal structures that can swell and contribute to obstruction.
Is Cottle’s classification outdated?
It’s still taught and referenced in many settings, but some experts prefer simplified segment descriptions because the five zones can be hard to apply consistently across all patients.
Use FAQs as a springboard for questions to discuss with your clinician, not as a self-diagnostic tool.
Summary + next step
If you’re dealing with persistent blockage, identifying where airflow is restricted—nostril vs nasal valve vs deeper cavity—can clarify why symptoms persist and which treatments are most likely to help. Frameworks like Cottle’s areas aren’t something you need to memorize, but they can explain why the same symptom (“congestion”) may require different approaches. If nasal obstruction is ongoing, worsening, or affecting sleep, consider an ENT evaluation and ask which area(s) seem involved. You can also ask how medical therapy compares with procedural options in your specific situation.
Location first, treatment second—that sequence keeps care targeted.
References
- Open-i (Cottle classification figure): https://openi.nlm.nih.gov/detailedresult?img=PMC4042609_1916-0216-43-11-2&req=4
- The ENT Resident – Cottle Areas teaching page: https://www.theentresident.com/ent-notes-lectures/cottle-area
- Huizing (2003) review figure reference (via ResearchGate): https://www.researchgate.net/figure/Areas-of-the-nose-according-to-Cottle-Area-1-nostril-Area-2-nasal-valve-Area-3-area_fig4_9038792
- Dillard J, Koudouovoh C, Lee V, et al. Rhinology Online. 2026;9:18–23. doi:10.4193/RHINOL/25.018
This article is for general education and isn’t a substitute for medical care.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.