

How We Use CT Scans to Evaluate Nasal Blockages
If you can’t breathe through your nose, a CT scan can sometimes help explain why—but not always. CT is excellent at showing structure (bone, sinus anatomy, narrow drainage pathways), but some causes of obstruction are dynamic (like nasal valve collapse that changes as you inhale) or primarily mucosal (swelling from allergies or irritation). Those problems may require other tools, such as an in-office exam, endoscopy, or functional tests.
This article explains when a nasal obstruction CT is most helpful, what it can and can’t show, how to think about radiation (including low-dose options), and what to ask your ENT. (Rhinology Journal Supplement 29, 2020)
What “Nasal Blockage” Really Means (And Why Diagnosis Can Be Tricky)
“Nasal blockage” is a symptom—not a diagnosis. Two people can describe the same “stuffy nose” feeling but have very different underlying causes. One person may have inflammation that fluctuates day to day; another may have a stable structural narrowing that’s been there for years.
A practical way to think about it: the nose is both a hallway (structure) and a set of curtains (lining). CT is great at mapping the hallway—walls, corners, and tight spots—but it’s less sensitive to how much the curtains are swelling or fluttering in real time.
Common symptom patterns patients notice
- One-sided vs. two-sided blockage (one nostril always worse, or alternating sides)
- Nighttime worsening (often worse when lying down) or symptoms that change with exercise
- Related symptoms like:
- Facial pressure or fullness
- Drainage/post-nasal drip
- Reduced sense of smell
- Headaches
- Sleep disruption or mouth breathing
Many ENTs start by listening for these patterns because they help predict which tools will be most informative. For example, “I’m fine at rest but worse during a run” can hint at a dynamic issue, while “pressure plus reduced smell for months” may fit chronic sinus inflammation. (Rhinology Journal Supplement 29, 2020)
Main categories of causes
ENTs usually think about nasal obstruction in a few broad buckets:
- Inflammatory: allergic rhinitis, nonallergic rhinitis, and chronic sinus inflammation
- Structural: deviated septum, turbinate enlargement, nasal polyps, and sinus anatomy variants
- Functional/dynamic: nasal valve collapse, where the narrowest part of the nasal airway partially closes during breathing or activity
If you suspect a deviated septum may be part of the problem, see deviated septum symptoms and treatment options: https://www.clearpathnasal.com/blog/deviated-septum-explained-symptoms-causes-and-modern-treatment-options
In short: CT maps structure well, but symptoms and real-time exam findings are essential to pinpoint the cause.

What a CT Scan Can Tell Us About Nasal Blockages
CT = “map” of the nose and sinuses (structure-focused)
A CT scan is essentially a detailed map of your nasal and sinus anatomy. It can show:
- Bony anatomy (septum, turbinates, sinus walls)
- How open the sinus air spaces are
- Key drainage pathways (where blockages can contribute to symptoms)
- Important anatomy variants that may affect symptoms or make surgery more complex
Clinicians often describe CT as a “roadmap” before navigating tight anatomy. It can also reveal complications of chronic sinus disease—when those complications are present—which is one reason it’s so valued in persistent or complex cases. (Rhinology Journal Supplement 29, 2020)
Why CT is widely used for chronic rhinosinusitis (CRS)
For chronic rhinosinusitis evaluation, CT is widely used and often preferred—especially when the diagnosis is unclear, symptoms persist despite treatment, or surgery is being considered. It helps identify findings consistent with chronic sinus inflammation, shows critical anatomy and anatomic variants, and supports safe, targeted surgical planning. (Rhinology Journal Supplement 29, 2020; AJR, 2022)
Bottom line: CT provides a high-resolution look at structure and sinus pathways, which is particularly useful when CRS is suspected or procedures are being planned.
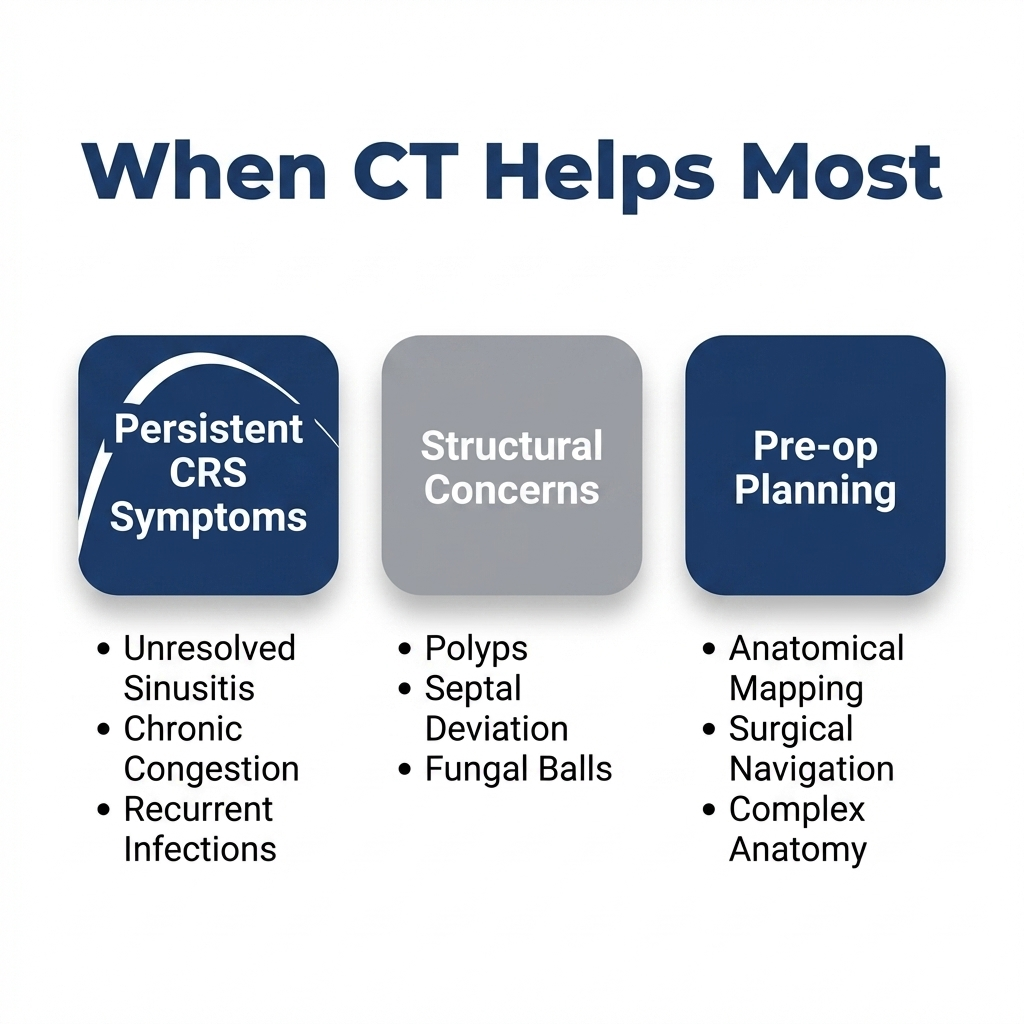
When CT Scans Are Most Helpful (Best-Use Scenarios)
ENTs don’t order CT scans for every stuffy nose. CT is most valuable when the results are likely to change the plan—clarifying anatomy, documenting disease, or guiding a procedure.
Chronic rhinosinusitis symptoms that persist
When symptoms last for weeks to months, keep coming back, or don’t improve with appropriate medical therapy, a sinus CT can help show whether findings consistent with chronic sinus inflammation are present and how extensive they are.
A concrete example: if someone has months of congestion plus facial pressure and reduced smell, CT may show which sinuses are involved and whether drainage pathways look narrowed—information that can steer medication choices or support a discussion about procedural options. (Rhinology Journal Supplement 29, 2020; AJR, 2022)
Pre-surgical planning (sinus surgery and some septal procedures)
CT is often used as a pre-operative roadmap—particularly if:
- Sinus surgery is being considered
- You have had prior nasal/sinus surgery (anatomy can change)
- Your clinician wants a clearer understanding of variants and “tight spaces” before operating
If you’re planning for combined procedures, you may find when septoplasty and sinus surgery are done together helpful: https://www.clearpathnasal.com/blog/septoplasty-and-sinus-surgery-when-they-aore-done-together
This planning role is one reason CT is closely linked with chronic sinusitis care; it helps the surgeon anticipate key landmarks and avoid surprises. (Rhinology Journal Supplement 29, 2020)
Suspected structural contributors (beyond “just congestion”)
CT can be especially helpful when the history and exam suggest structural narrowing, such as:
- Concha bullosa (an air-filled middle turbinate that can crowd airflow)
- Turbinate hypertrophy patterns
- Septal spurs
- Narrowed sinus outflow areas
When you’re trying to separate “swelling” from “shape,” a deviated septum CT and sinus CT views can add clarity—though CT still needs to be interpreted alongside symptoms and physical exam findings. For more on next steps if structure may be part of the problem, see what to do next if chronic congestion may be structural: https://www.clearpathnasal.com/blog/deviated-septum-and-chronic-nasal-congestion-what-to-do-next
Takeaway: Order CT when the result will change management—particularly for persistent CRS symptoms, structural concerns, or pre-op mapping.

When CT Scans Are Not Routinely Recommended
Acute rhinosinusitis (short-term sinus infection)
For uncomplicated acute sinusitis, CT is usually not recommended as a routine step. Many cases improve with time and appropriate medical care, and imaging may not change treatment.
Another downside: CT can show incidental findings (like mild mucosal thickening) that sound alarming on paper but aren’t actually driving symptoms—leading to confusion or unnecessary worry. (AJR, 2022)
Isolated septal deviation or internal nasal valve concerns
CT can show septal shape, but it may not fully explain airflow—especially at the internal nasal valve, the narrowest part of the nasal airway. CT findings can correlate poorly with what’s seen on physical exam of the nasal valve and with real-world breathing symptoms. (Rhee et al., 2005)
Because CT is a static test, collapse that happens only during inhalation or exercise may be missed on a still image. Exam-based techniques often provide more insight in suspected valve dysfunction.
In brief: For short-term infections and purely dynamic valve issues, CT usually adds little to initial decision-making.

CT vs. Other Tests: What Each One Adds
Nasal endoscopy (often the most direct look)
In many cases, endoscopy is one of the most practical and informative tools. It allows an ENT to directly visualize:
- Swelling and inflammation patterns
- Polyps
- Drainage
- Areas of narrowing
- Dynamic changes during breathing maneuvers
Because endoscopy is done in real time, it can capture what CT cannot—for instance, a segment that collapses only during inhalation or only when the patient sniffs. (Rhee et al., 2005)
Functional testing for nasal valve collapse (when breathing feels worse with activity)
CT can show structural contributors, but if collapse happens primarily during inhalation, exercise, or certain positions, dynamic assessment is important. ENTs may use:
- Endoscopy during breathing maneuvers
- Adjunctive functional testing such as acoustic rhinometry, which helps measure nasal airway dimensions and changes; availability may vary by clinic (Rhee et al., 2005)
A common “tell” is the patient who says, “I can breathe until I take a deep breath,” or “It’s worse when I’m active.” That’s often a cue to look beyond a static scan.
Allergy evaluation and medication trials (when swelling is the driver)
If swelling is the main issue, imaging doesn’t replace treatment. Allergy evaluation and appropriate medication trials (and sometimes environmental changes) are often the most direct path to improvement. CT may still be useful later if symptoms persist or if chronic sinusitis becomes a concern. (Rhinology Journal Supplement 29, 2020; AJR, 2022)
Summary: Endoscopy adds real-time insight, functional tests assess dynamic airflow, and allergy care targets mucosal swelling—complementing, not replacing, CT.

Understanding Radiation and Safety (Especially for Children)
Why radiation dose matters
CT uses ionizing radiation, so dose matters—particularly for children, who are more sensitive to radiation effects. A good general approach is to image only when results are likely to change management, and to tailor technique to the clinical question. (AJR, 2022)
Low-dose CT and cone-beam CT (CBCT): what patients should know
Many centers use low-dose sinus CT protocols when appropriate, especially for sinus evaluation and surgical planning. Another option you may hear about is cone-beam CT (CBCT).
CBCT can reduce radiation dose in certain contexts, but it typically has limited soft-tissue detail—important when the main question is inflammation versus structure. It is not equivalent to standard CT for every sinus question. (Rhinology Journal Supplement 29, 2020; AJR, 2022)
Questions to ask your clinician about dose and necessity
- Will this scan change the treatment plan?
- Is a low-dose sinus CT appropriate for me?
- Should we do endoscopy first?
- If this is for surgical planning, what specifically are you looking for?
Key point: Use the lowest reasonable dose for the clinical question, and image when results are likely to guide care.
What to Expect If Your ENT Orders a Sinus CT
How the scan is performed
A sinus CT is fast and noninvasive. In most cases:
- You lie still on a table for a brief scan
- No needles are typically needed
- Contrast is usually not required for routine sinus CT
Some patients worry they’ll feel “closed in,” but sinus CT is typically quick, and the scanner does not usually require long time inside a tunnel.
How results are read (and why symptoms still matter)
CT provides valuable anatomy and inflammation information, but it’s only one piece of the puzzle. Your clinician typically combines:
- Your symptom history (timing, triggers, severity)
- Nasal exam and/or endoscopy findings
- Response to medications
- CT results (Rhinology Journal Supplement 29, 2020; AJR, 2022)
This combined approach helps avoid over-treating incidental CT findings and keeps the focus on what is actually driving symptoms.
Remember: CT findings should be interpreted alongside your symptoms and exam—not in isolation.
How CT Findings Can Guide Treatment Options
Medical management when inflammation dominates
When CT and exam suggest inflammation is the main driver, treatment often focuses on:
- Saline irrigation
- Nasal steroid sprays
- Allergy management when relevant
- Targeted antibiotics only when indicated for specific situations
CT doesn’t replace these steps—it helps show where inflammation is likely present and whether anatomy might be contributing to poor drainage. (Rhinology Journal Supplement 29, 2020)
Procedure/surgery planning when structure contributes
When structure is a significant contributor—such as septal deviation, spurs, turbinate enlargement, or chronic sinus blockage—CT can guide planning by clarifying anatomy and showing the extent of disease. For patients who have both sinus and septal issues, see how septoplasty can fit into chronic sinusitis treatment: https://www.clearpathnasal.com/blog/the-role-of-septoplasty-in-treating-chronic-sinus-sinusitis
If you’re evaluating septal deviation specifically, this guide can help with patterns and next steps: deviated septum symptoms and treatment options: https://www.clearpathnasal.com/blog/deviated-septum-explained-symptoms-causes-and-modern-treatment-options
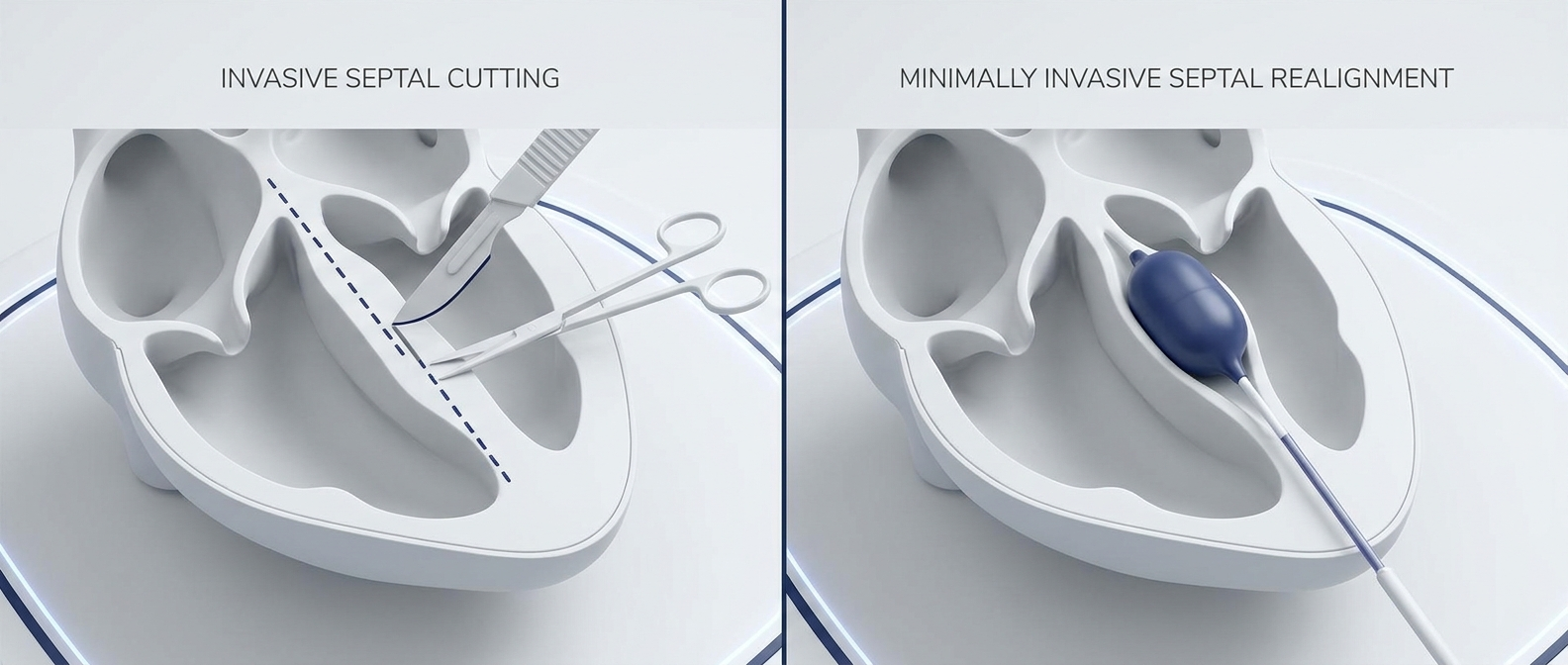
Where minimally invasive septal approaches may fit (brief, non-promissory)
In some practices, CT can also document septal anatomy before and after device-assisted septoplasty approaches such as those using the ClearPath system. Early retrospective data suggest that outcomes may improve in some patients, but larger, controlled studies are needed to confirm benefit and safety. For example, a retrospective series of 107 consecutive device-assisted septoplasty cases reported that among 23 patients with pre- and post-operative CT scans, septal alignment improved by 22% at the nasolacrimal duct landmark and 45% at the point of maximal deviation; in a subgroup with SNOT-22 scores, averages improved from 58.7 to 44.8 at one month. No major complications were reported in that cohort. These findings are preliminary and should not be interpreted as proof of superiority over standard approaches. (Dillard et al., 2026)
If you’re comparing approaches, see ClearPath vs Traditional Septoplasty (recovery/safety/results): https://www.clearpathnasal.com/blog/clearpath-vs-traditional-septoplasty-recovery-safety-results and ask your local ENT whether any approach is appropriate for your specific anatomy and diagnosis.
Practical note: When structure drives symptoms, CT helps tailor procedural planning—while dynamic valve function and mucosal drivers still require exam-based assessment.
FAQs About CT Scans for Nasal Obstruction
“Will a CT scan show why I can’t breathe through my nose?”
Often, yes—especially for chronic sinus disease and many structural issues. But CT is less reliable for dynamic problems like nasal valve collapse, where airflow changes during breathing. That’s one reason CT is frequently paired with endoscopy and, when needed, functional testing. (Rhinology Journal Supplement 29, 2020; Rhee et al., 2005)
“Do I need a CT scan before septoplasty?”
Not always. If symptoms and exam strongly suggest isolated septal deviation (or internal nasal valve dysfunction), CT may not be routinely indicated. If chronic sinusitis is suspected, prior surgery changed anatomy, or combined planning is needed, CT can be more helpful. For more background on next steps, see deviated septum symptoms and treatment options: https://www.clearpathnasal.com/blog/deviated-septum-explained-symptoms-causes-and-modern-treatment-options (AJR, 2022; Rhee et al., 2005)
“Is cone-beam CT just as good?”
It depends on the clinical question. Cone-beam CT (CBCT) can be useful for certain structural evaluations and may lower dose, but its soft-tissue detail is more limited—important when evaluating inflammation. (Rhinology Journal Supplement 29, 2020; AJR, 2022)
Key Takeaways + Next Steps
- CT is most helpful when chronic rhinosinusitis is suspected or when surgical planning is on the table.
- CT is usually not needed for uncomplicated acute sinus infections and can be limited for purely functional nasal valve problems.
- Ask about radiation dose and whether low-dose CT, endoscopy, or functional testing (like acoustic rhinometry) should come first.
- If nasal blockage is affecting sleep, exercise, or daily life, schedule an ENT evaluation to pinpoint the cause and build a plan—and ask your local ENT whether traditional surgery or minimally invasive approaches (including device-assisted techniques, when appropriate) fit your situation.
Medical disclaimer: This article is for general educational purposes only and is not medical advice. Imaging choices and treatment decisions should be made with a qualified clinician who can evaluate your symptoms and exam findings.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
References
- Rhinology Journal Supplement 29 (2020). https://www.rhinologyjournal.com/Documents/Supplements/supplement_29.pdf
- American Journal of Roentgenology (2022) (via JACR). https://www.jacr.org/article/S1546-1440(22)00181-8/fulltext
- Rhee JS, et al. Nasal Valve Obstruction Review (2005). https://pmc.ncbi.nlm.nih.gov/articles/PMC11983596/
- Dillard J, Koudouovoh C, Lee V, et al. Rhinology Online. 2026;9:18–23. doi:10.4193/RHINOL/25.018
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.