

Chronic Headaches and Nasal Spurs: Is There a Connection?
Headaches are common and often blamed on “sinuses” or labeled as migraines. But for a subset of people, the real driver can be inside the nose: a deviated septum with a nasal spur. If you’ve been dealing with ongoing facial pressure, one-sided nasal blockage, and headaches that don’t fully respond to typical treatments, it’s worth understanding the link between chronic headaches and nasal spurs.
Think of it like a door that doesn’t swing cleanly. Sometimes the problem isn’t the room (your “sinuses”)—it’s the doorframe (your nasal anatomy) rubbing in just the wrong spot, over and over, until it becomes painful.
Quick Answer—Yes, Sometimes (And It’s Often Missed)
Not all headaches are sinus-related. In fact, many “sinus headaches” turn out to be migraine or another primary headache disorder. Still, nasal anatomy can contribute to headaches in some patients, especially when there’s significant narrowing or a painful contact point inside the nasal cavity.
Here are the key terms in plain language:
- Nasal spur: A small bony projection, often along the nasal septum, commonly associated with a deviated septum.
- Deviated septum: When the thin wall (septum) between your nostrils is off-center, making one nasal passage smaller. Cleveland Clinic: https://my.clevelandclinic.org/health/diseases/16924-deviated-septum
- Rhinogenic headache / mucosal contact point headache: Head pain believed to be triggered by nasal structures touching and irritating sensitive nasal lining and nerves. Healthline: https://www.healthline.com/health/headache/rhinologic-headache
This overlap is a big reason chronic headaches and nasal spurs can be missed: symptoms may look like “migraine,” “sinus pressure,” or both. A patient might say, “It feels like sinus pressure behind my eye,” while the root cause may be structural narrowing, mucosal irritation, or a combination of factors.
Conclusion: It’s possible for nasal anatomy and primary headache disorders to overlap, so a careful evaluation matters.
Nasal Spurs 101—What They Are and Why They Can Hurt
What is a nasal spur?
A nasal spur is typically a sharp or shelf-like bony prominence that forms along the septum. It often develops due to:
- A deviated septum (from growth patterns or longstanding asymmetry)
- Prior nasal trauma
- Natural changes in cartilage/bone alignment over time
For a more detailed overview of deviated septum symptoms, causes, and treatment options, see: deviated septum symptoms, causes, and treatment options https://www.clearpathnasal.com/blog/deviated-septum-explained-symptoms-causes-and-modern-treatment-options
Common symptoms that can travel beyond the nose
Nasal spurs are often thought to cause only congestion, but they may also contribute to:
- One-sided nasal blockage (often persistent)
- Facial pressure/fullness
- Postnasal drip
- Recurrent “sinus” complaints (even without true infection)
- Headaches described as:
- Pressure behind the eyes
- Cheek or forehead pain
- A “tight band” or heavy feeling in the face
A practical example: someone may notice they can breathe well on the right but poorly or not at all on the left—then, during allergy season or a cold, the left side closes down further and the headache pattern flares with it.
MedicalNewsToday provides a helpful consumer overview of the deviated septum–headaches connection: https://www.medicalnewstoday.com/articles/deviated-septum-and-headaches
Cleveland Clinic summarizes common deviated septum symptoms and impact: https://my.clevelandclinic.org/health/diseases/16924-deviated-septum
Conclusion: Spurs and deviation can drive symptoms beyond congestion, including facial pressure and headache.

The Two Main Pathways Linking Nasal Spurs/Deviated Septum to Chronic Headaches
Pathway #1 — Obstruction → Poor drainage → Inflammation → “Sinus headache” symptoms
When a septum is significantly deviated—or when a spur narrows airflow—your nasal passages may not ventilate as effectively. In some people, that narrowing is associated with:
- Persistent congestion
- Reduced sinus ventilation/drainage
- Inflammation that creates facial pressure and pain
This can resemble a “sinus pressure” headache, especially when symptoms cluster around the cheeks, forehead, or behind the eyes. Importantly, this doesn’t always mean you have a bacterial sinus infection; inflammation alone can cause pressure and discomfort. Mayo Clinic sinusitis symptom context: https://www.mayoclinic.org; PMC discussion: https://pmc.ncbi.nlm.nih.gov/articles/PMC4835330/
A helpful analogy: swelling in a narrow nasal passage can behave like a kinked garden hose—flow becomes inefficient, pressure sensations increase, and symptoms can ramp up even without “infection.”
Pathway #2 — Mucosal contact point headaches (the “direct trigger”)
The second pathway is often discussed in the context of mucosal contact point headache (also called rhinogenic headache). The idea is straightforward:
- A spur or sharply deviated septum can touch the lateral nasal wall or a turbinate
- That contact can irritate the nasal lining (mucosa) and stimulate sensory pathways
- Pain can be “referred” to the forehead or around/behind the eyes due to trigeminal nerve connections
This is a recognized concept in ENT literature, though diagnosis can be complex and is often considered after ruling out other causes. PMC overview: https://pmc.ncbi.nlm.nih.gov/articles/PMC7253539/; classic reference: https://pubmed.ncbi.nlm.nih.gov/8084628/
For more on how septoplasty may relieve pressure when anatomy is a driver, see: deviated septum headaches and septoplasty relief https://www.clearpathnasal.com/blog/deviated-septum-headaches-how-septoplasty-can-relieve-pressure
Conclusion: Nasal anatomy can trigger pain either indirectly via inflammation or directly via mucosal contact.

Why These Headaches Are Commonly Mistaken for Migraines
Overlapping symptoms (and why that matters)
Migraine and nasal/sinus-related pain can overlap. Some people with facial pressure also report:
- Light sensitivity
- Nausea
- A sense of “sinus pressure” without infection
Many people self-diagnose “sinus headaches,” when migraine is actually the cause (or part of the cause). Healthline reviews this overlap: https://www.healthline.com/health/headache/rhinologic-headache
A common real-world scenario: someone is treated repeatedly with antibiotics for “sinus headaches,” but the pattern keeps returning—because the core issue may be migraine, nasal anatomy, or both.
Clues that point toward a nasal structural cause
Consider asking for an evaluation by an Ear, Nose, and Throat (ENT) specialist when headaches occur alongside:
- Consistent nasal blockage, especially worse on one side (Cleveland Clinic: https://my.clevelandclinic.org/health/diseases/16924-deviated-septum)
- Headache/facial pressure that worsens during colds, allergy flares, or congestion periods
- Symptoms that feel linked to airflow (for example, worse when one side is more swollen)
- History of nasal trauma, chronic mouth breathing, snoring, or recurrent sinus complaints
For more on the overlap between sinus symptoms and migraine, see: sinus pressure headache vs migraine—how septoplasty may affect both https://www.clearpathnasal.com/blog/how-septoplasty-impacts-sinus-headaches-and-migraines
Conclusion: Because symptoms overlap, ruling in or out nasal contributors can prevent misdiagnosis and repeat treatments that don’t help.
How ENTs Confirm the Diagnosis (What Patients Can Expect)
Key history questions your clinician may ask
A good evaluation usually starts with patterns and triggers, such as:
- How often headaches happen and how long they last
- Whether pain correlates with congestion or seasonal allergies
- Response to migraine-directed medications vs. nasal therapies
- Frequency of sinus infections (and whether they were confirmed)
You might hear questions like: “Do you feel pressure mostly around one eye?” or “Do symptoms reliably worsen when your nose is blocked?” Those details help separate structural contributors from primary headache disorders.
Nasal exam + nasal endoscopy
A nasal endoscopy is a small-camera exam done in the office. It can help an ENT visualize:
- Septal deviation and spurs
- Inflammation
- Potential contact points (septum-to-turbinate contact)
- Other contributors to obstruction
When CT imaging is helpful
CT imaging can be useful when the goal is to:
- Evaluate for chronic sinus disease
- Map the location and severity of deviation/spurs
- Support surgical planning when appropriate
Diagnostic approach discussion: https://pmc.ncbi.nlm.nih.gov/articles/PMC6391278/
Deviated septum basics: https://my.clevelandclinic.org/health/diseases/16924-deviated-septum
Conclusion: A targeted ENT exam—often with endoscopy and sometimes CT—clarifies whether anatomy plays a meaningful role.

Treatment Options—From Conservative Relief to Structural Fix
Step 1 — Treat inflammation and contributing factors first
Many people benefit from addressing inflammation before considering procedures. Depending on your situation, a clinician may recommend:
- Saline rinses
- Allergy management
- Nasal steroid sprays (when appropriate)
- Treatment of sinusitis if present and confirmed
These can reduce swelling and improve airflow—but they cannot remove a bony spur or permanently eliminate an anatomic contact point. Cleveland Clinic management context: https://www.clevelandclinic.org/health/diseases/16924-deviated-septum
Step 2 — When surgery becomes the most effective option
If symptoms strongly correlate with anatomy—and headaches persist despite appropriate medical therapy—surgery may be discussed. Options can include:
- Septoplasty (to straighten the septum and address spurs when clinically indicated)
- Turbinate reduction (when indicated)
- Sinus procedures if chronic sinusitis is present
Not all nasal spurs require surgery or cause symptoms; treatment decisions depend on symptom correlation and clinical evaluation. While mucosal contact point headache is a recognized concept, diagnosis can be nuanced and is typically considered after other causes are evaluated.
Conclusion: Start with medical therapy; consider procedures only when symptoms clearly align with treatable anatomy.
Septoplasty and Headache Relief—What the Evidence Suggests
Many patients improve—especially when anatomy is clearly involved. Studies and clinical reviews often report improvement in facial pain/headache symptoms after correcting obstruction or contact points—when patients are carefully selected and the headache mechanism fits the nasal findings. PMC discussion: https://pmc.ncbi.nlm.nih.gov/articles/PMC7253539/
Realistic expectations: Even with a clear structural issue, surgery isn’t a guaranteed “cure-all.” Many patients see reduced frequency or intensity, but headaches can be multi-factorial. Some people may experience both anatomy-driven facial pressure and a primary headache disorder, such as migraine. Coordinated care (ENT + primary care/neurology) can be helpful. Balanced overview: https://www.medicalnewstoday.com/articles/deviated-septum-and-headaches
For additional context on outcomes and selection, see: deviated septum headaches and septoplasty relief https://www.clearpathnasal.com/blog/deviated-septum-headaches-how-septoplasty-can-relieve-pressure
Conclusion: Septoplasty is most helpful when your symptom pattern (“why”) matches what the ENT sees on exam or imaging (“what”).

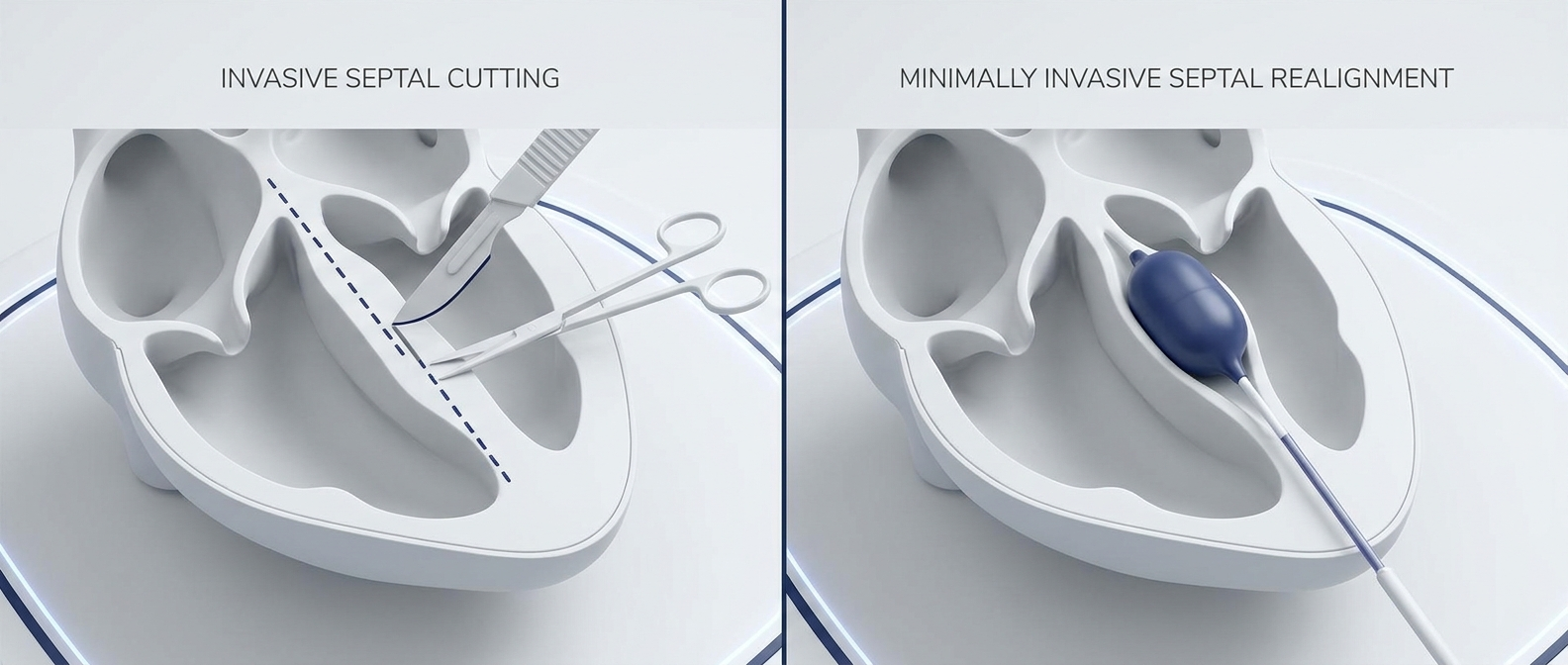
A Minimally Invasive Option: Balloon-Assisted Endoscopic Septoplasty (ClearPath Context)
Balloon-assisted techniques are one modern approach ENTs may consider for selected patients. ClearPath is a device used in force-directed balloon-assisted endoscopic septoplasty, performed under endoscopic visualization.
What “balloon-assisted septoplasty” means (in everyday terms)
In general terms, this approach uses controlled pressure to help mobilize and reposition portions of a deviated septum. The goal is to improve airflow and reduce problematic narrowing/contact—while potentially simplifying certain steps compared with more extensive flap elevation in some cases.
To learn the basics, see: What is balloon septoplasty? https://www.clearpathnasal.com/blog/what-is-balloon-septoplasty-a-minimally-invasive-option-for-deviated-septum
What early outcomes show (ClearPath Nasal Balloon study highlights)
- 107 cases were reported with no major complications observed in that series (no septal perforation, hematoma, mucosal injury, or synechia reported).
- In 23 patients with pre/post CT scans, there was 45% mean improvement at the point of maximal deviation and 22% improvement at the nasolacrimal duct (p = 0.005).
- Symptoms improved: SNOT-22 decreased by ~24%, including notable improvements in nasal congestion, headache/facial pressure, and sleep at ~1 month.
- The technique may streamline steps (less flap elevation/packing/suturing in some cases), potentially reducing procedural/anesthesia time.
Citation: Dillard JD, Koudouovoh C, Lee V, et al. Outcomes of force-directed balloon-assisted endoscopic septoplasty: a retrospective analysis with a new technique and device. Rhinology Online. 2026;9:18–23. http://doi.org/10.4193/RHINOL/25.018
While early reports are promising, this evidence comes from a retrospective series; individual results vary, and patients should review risks, benefits, and alternatives with their surgeon.
Conclusion: Balloon-assisted techniques may suit selected anatomies, but candidacy and expectations should be individualized.
When to See a Doctor (And When to Seek Urgent Care)
Make an ENT appointment if you have…
- Chronic or recurrent headaches plus ongoing nasal obstruction
- “Sinus headaches” that don’t follow typical infection patterns
- Headache/facial pressure plus snoring, poor sleep, or mouth breathing
Seek urgent care for red flags
Get urgent evaluation for:
- Sudden severe “worst headache”
- New neurologic symptoms (weakness, confusion, trouble speaking)
- Vision changes
- High fever with stiff neck
- Headache after head injury
Mayo Clinic general guidance: https://www.mayoclinic.org
Conclusion: Don’t ignore red flags—seek urgent care when severe or new symptoms appear.
FAQs
Can a nasal spur really cause headaches?
Yes, sometimes. Chronic headaches and nasal spurs may be linked through (1) obstruction with inflammation/pressure and (2) mucosal contact point headache mechanisms where a spur irritates sensitive nasal lining and referred nerve pathways. Healthline: https://www.healthline.com/health/headache/rhinologic-headache; PMC: https://pmc.ncbi.nlm.nih.gov/articles/PMC7253539/
How do I know if it’s a migraine or a sinus/nasal headache?
Symptoms overlap, and mislabeling is common. Migraine can look like “sinus pressure,” and nasal structural issues can mimic migraine-like facial pain. A careful history plus ENT exam (and sometimes CT) is often the clearest way to sort out sinus pressure headache vs migraine and identify nasal contributors.
Will septoplasty cure my headaches?
Not guaranteed. Septoplasty for headaches tends to help most when the headache pattern aligns with obstruction or a clear contact point on exam/imaging. Some people improve significantly; others have partial improvement, especially if migraine is also present. PMC: https://pmc.ncbi.nlm.nih.gov/articles/PMC7253539/; MedicalNewsToday: https://www.medicalnewstoday.com/articles/deviated-septum-and-headaches
What tests diagnose a mucosal contact point headache?
There’s no single “one-test” diagnosis. ENTs typically use:
- Symptom history and triggers
- Nasal exam/endoscopy
- CT imaging when helpful for anatomy and sinus evaluation
Healthline: https://www.healthline.com/health/headache/rhinologic-headache; PMC: https://pmc.ncbi.nlm.nih.gov/articles/PMC6391278/
Conclusion: A structured evaluation helps distinguish migraine from anatomy-driven pain and guides the right treatment.
Conclusion—Treat the Cause, Not Just the Pain
Chronic headaches and nasal spurs can be related—most often through obstruction/inflammation or through direct mucosal contact point irritation. Because these symptoms can look like migraine or “sinus headaches,” the problem is easy to miss without a targeted nasal evaluation.
CTA: If your headaches reliably show up with congestion, one-sided blockage, facial pressure, or sleep disruption, schedule an evaluation with a qualified ENT and ask whether your nasal anatomy—including spurs, deviation, and potential contact points—could be contributing. If procedures are on the table, you can also ask whether minimally invasive options such as ClearPath are appropriate for your case.
This article is for educational purposes only and is not medical advice. Please consult a qualified healthcare provider for diagnosis and treatment.
Contact
.webp)
Dr. David Dillard
Resent posts





Contact us
Have questions about the ClearPath Nasal Balloon System? Our team is here to help with product inquiries, demonstrations, or order support.